
Stick A Fork In It
The Barbecue Rebellion & The Rude Awakening


In March 2021, Risk It For The Brisket: The Barbecue Rebellion & The Great Reject told the story of William Adamson (Adam) Skelly and the justification for his valiant stand against unproven covid measures. He was arrested in November 2020 for the ‘crime’ of opening his restaurant during the second wave of lockdowns. For his civil disobedience, Canadian bureaucrats and media took him to task. They painted him as a virulent villain, ignoring the righteous rationale for his rebellion. On reply, he lodged a constitutional challenge to the Reopening Ontario Act, the basis upon which all provincial covid mandates and restrictions were – and in some instances, still are – implemented.
Standing on sensible scientific expertise and Canada’s Charter Rights, his challenge went to court in June 2021, but no sooner than the hearing began did the case get turned away due to a procedural error. Months of preparation, expert witness testimony, cross-examinations, and other legal submissions were summarily dismissed, delaying a momentous opportunity to expose the fallacies underlying the government’s response to covid. Undeterred, Skelly has filed a revised challenge. Although many who previously supported the harmful measures and exhibited repressive behaviours have since changed their tune, there is a stark difference between those offering a sincere apology with admission of grave error, and those making pleas for amnesty with no regret or remorse. The former is welcome, but the latter rings hollow because the bell tolls for accountability, not absolution.
It's been three years since covid emerged. In their panicked response, public officials discarded tried-and-true principles of governance and healthcare, giving way to untested and extreme restrictions. With no regard for the social contract and democratic processes, nor the collateral damage of breaking them, the prevention of covid became the driving force behind all institutional decision-making. And yet, despite the many predictable harms inflicted on a broad range of Canadians, no formal risk-benefit analysis of the government’s actions was ever conducted, and no court has heard a comprehensive repudiation of them. This is where Skelly’s case comes in – it mounts a justifiable offensive against the purported premises underpinning all covid measures.
“We’re challenging the Reopening Ontario Act in its entirety. We’re going to be challenging all of the evidence that supports what’s left of this pandemic narrative, and whether or not it infringes on our Charter… This will be the most vast and broad challenge against the emergency orders in the country.”
All told, six subject matter experts provided reports in April 2021 testifying on topics such as diagnostics, economics, medicine, public health, statistics, epidemiology, and more. The evidence they submitted cannot be reviewed in its entirety – that will occur in the courtroom – but some of the key premises can, especially in the context of our lived experience. To that end, the following topics will be covered (click on any to skip to a specific section, or continue reading):

Principles of Public Health
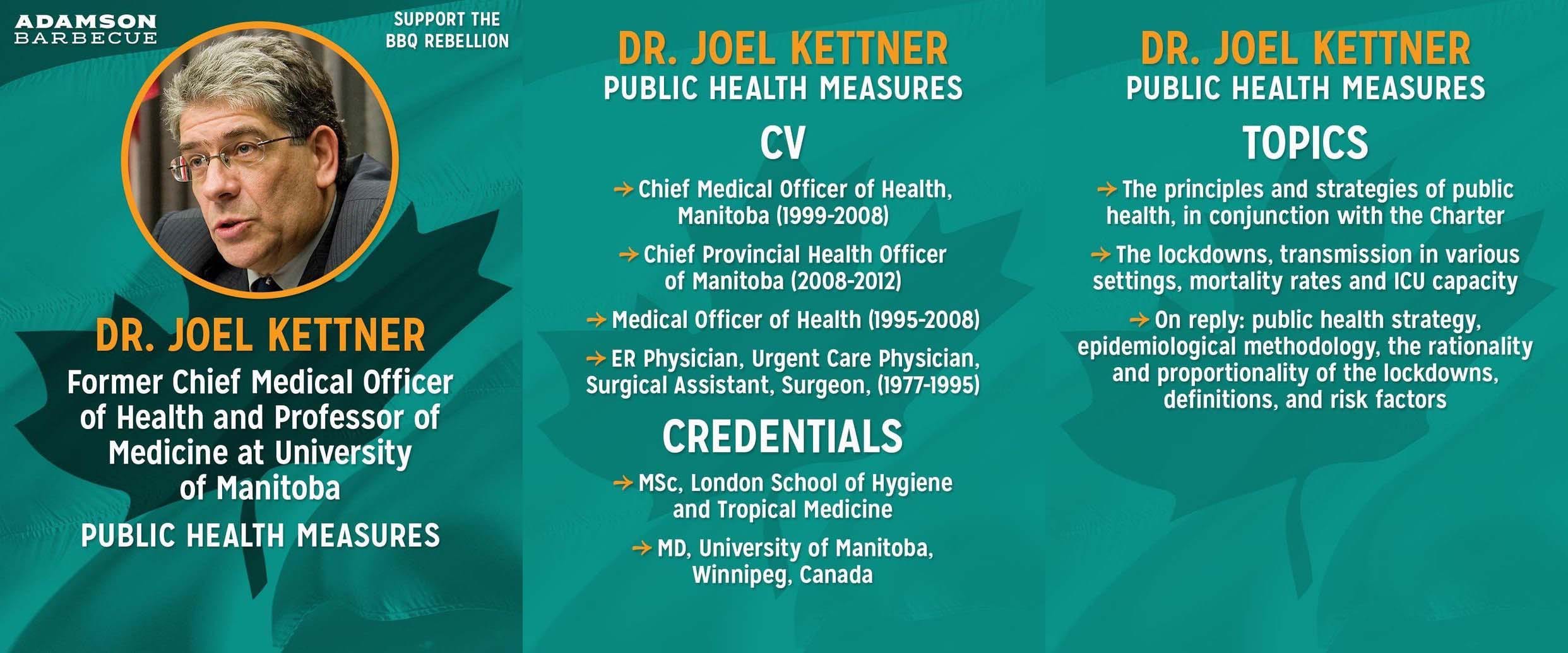
To begin, consider witness Dr. Joel Kettner, former Chief Medical Officer of Health for Manitoba and professor at University of Manitoba. He was called upon to discuss the principles and strategies of public health. In his affidavit, he reminded Canadians that “in a public health emergency, the advice from public health professionals is expected to be based on valid and reliable data, relevant information, objective scientific evidence, and critical reasoning.”
Remember the initial “two weeks to flatten the curve,” which was the precursor for extended lockdowns? Can you recall what reliable data and objective evidence informed that approach? No, you can’t, because there was none. Lockdowns were a knee-jerk reaction that gained traction due to two primary factors:
A speculative epidemiological model by Neil Ferguson et al, which was hastily given credence by the World Health Organization (WHO) and international media despite Ferguson’s abysmal track record modelling the 2005 bird flu and 2009 swine flu outbreaks, among others.
A visit to China by Dr. Clifford Lane of the National Institute of Health (NIH), who reported being “very impressed” with the country’s ruthless restrictions despite their “great cost.” His claim was bolstered by a sophisticated propaganda campaign out of China, which used social media to push unsubstantiated claims of “success” in containing the virus, popularizing lockdowns in the susceptible minds of a frightened public.
Prompted by conjecture, hearsay, and misinformation, the profession tasked to think and act on verifiable fact – public health – succumbed to peer pressure, circumvented peer review, and blindly followed the leads of a disgraced forecaster and a notoriously opaque nation. Unfortunately, this was merely their first failure on what proved to be a very slippery slope.
“We have heard from federal, state, and even local officials that Chinese diplomats are aggressively urging support for China’s handling of the COVID-19 crisis. Yes, this is happening at both the federal and state levels… We had a state senator who was recently even asked to introduce a resolution supporting China’s response to the pandemic.”
– Christopher Wray, Director of the Federal Bureau of Investigation (FBI). July 7, 2020.
Continuing with Dr. Kettner’s testimony, he explained that “decisions must consider short-term and long-term benefits and harms for society as a whole. These considerations must include all matters pertaining to health. Even when one specific disease becomes the focus of attention, decision-makers and advisors must consider… the causes and risk factors of all diseases and injuries. These factors are often referred to as determinants of health.” Past pandemic plans understood these concepts and accounted for them. In fact, according to Health Canada’s Pandemic Influenza Preparedness Guidance for the Health Sector from December 2018, lessons learned from the 2009 H1N1 pandemic include:
“The public health benefits of any given measure must be weighed against the economic and social costs of its implementation.”
“The rationales for implementing them must be clear and consistently communicated to the public and updated as the situation evolves.”
“Widespread restrictions of movement to contain or slow an emerging pandemic are impractical, if not impossible, to implement.”
“International border entry screening is ineffective… at best it can delay epidemics by only a few weeks.”
Retired Lieutenant Colonel David Redman, a 27-year veteran who wrote Alberta’s 2005 pandemic preparedness influenza response plan and was the former head of the Alberta Emergency Management Agency, tried diligently to remind Canada’s leaders of these and other lessons. In a January 2021 interview, he said “governments took every emergency pandemic plan they’d ever written and threw them out the window when COVID arrived.” In another interview, in February 2023, he explained that the failure of elected officials to use the plans should make them guilty of “incompetence because they did not do their due diligence.” Throughout covid, he wrote letters to all provincial premiers advising them how and why their approach was misguided and urging them to change course, but he only received automatic replies and was never brought in for consultation.
His input would have been especially valuable because he understood how all areas of society are impacted by emergency restrictions, having factored feedback from all sectors – not just healthcare – into the pandemic plans. As such, he further criticized premiers for deferring to medical doctors, not provincial emergency management offices, for final say on decision-making. Why not defer to doctors? Because it’s like asking soldiers in the trenches how the war is going. Doctors, like soldiers, play a vital role and have a valuable skillset, but they are purpose-specific, and lack the perspective, preparation, and experience, to address critical issues affecting the needs of society at large.
Thinking back on the heavy-handed restrictions throughout covid, was public health’s narrow obsession with avoiding the virus truly in everyone’s best interests? Were any alternative strategies considered, especially ones that would have been less damaging and accounted for all determinants of health? Were measures proportional to risk? Was public health messaging consistent and logical? When new evidence emerged, was it clearly communicated to the public and were measures updated accordingly? Were lessons of past pandemics factored into decision-making? Regrettably, the answer to all these questions is a resounding ‘no.’
“Lockdown was never part of our planned pandemic response, nor is it supported by strong science… Our well-intentioned but misguided efforts to control Covid are only compounding the tragedy. We need to change course. No one has all the answers, but the first step is asking the right questions.”
– Dr. Richard Schabas, Former Chief Medical Officer of Health of Ontario. January 18, 2021.

Lockdowns & Censorship
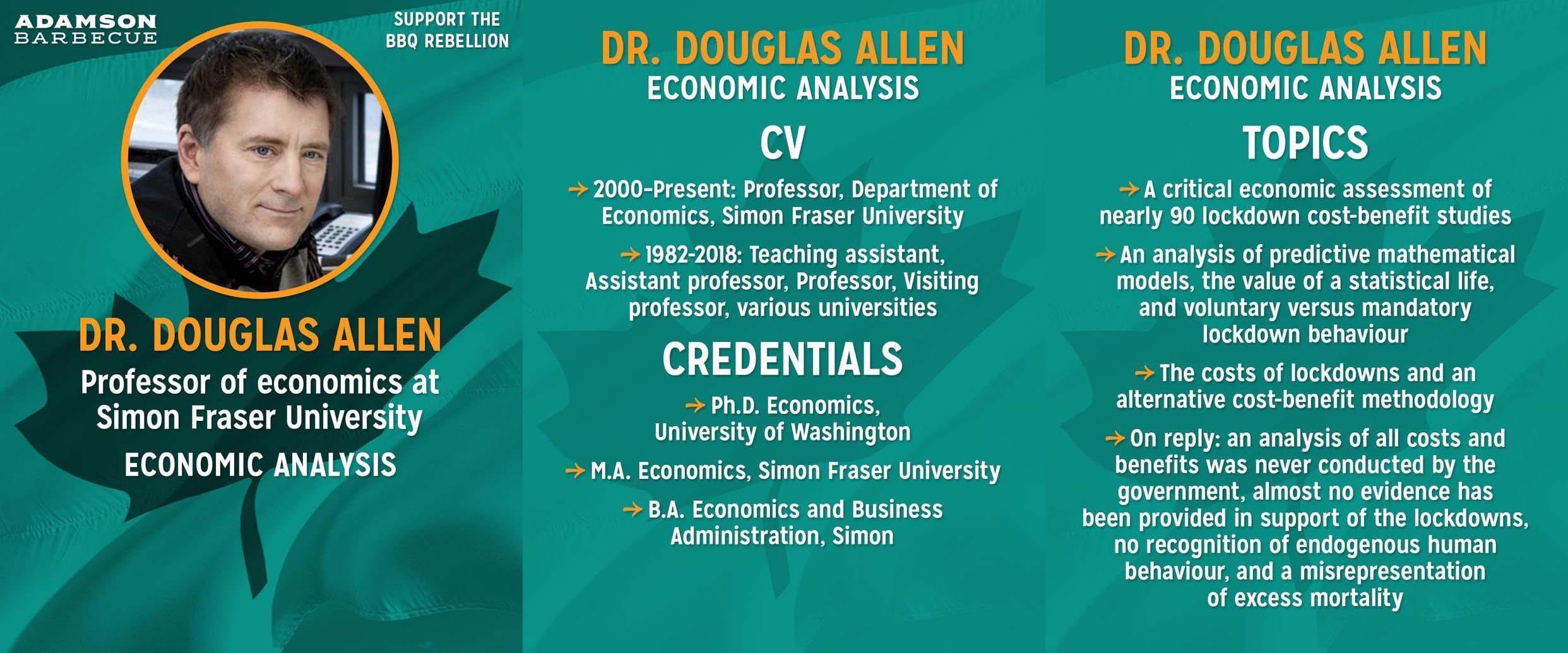
Witness Dr. Douglas Allen, professor of economics at Simon Fraser University, noted that the “early cases made for lockdown rested on several unrealistic assumptions,” with the majority of research focused on benefits and scant attention paid to costs. This might explain public health’s initial assumption that lockdowns were worthwhile, but according to Dr. Allen, “by August [2020] there was enough information available to show that any reasonable cost/benefit analysis would show that lockdown was creating more harm than good. It is unreasonable to suggest that a proper decision could not have been made in the fall when the second wave of infections hit.” He also famously wrote, “it is possible that lockdown will go down as one of the greatest peacetime policy failures in Canada’s history,” because, as he foresaw, the collateral damage from lockdowns was substantial. In hindsight, most would agree.
In the moment, however, only a few dared to advocate for a lighter touch. Among them were several renowned epidemiologists, including Harvard’s Dr. Martin Kulldorff, Oxford’s Dr. Sunetra Gupta, and Stanford’s Dr. Jay Bhattacharya. On October 4, 2020, they published the Great Barrington Declaration (GBD) – a formal proposal outlining an approach to covid that they called “Focused Protection.” Co-signed by over 63,000 medical practitioners and health scientists, it cautioned policymakers about the devastating short- and long-term physical and mental effects of oppressive covid restrictions. Furthermore, it emphasized key facts that had since come to light, which should have been cause for course correction, such as:
Covid is mostly a threat to the elderly and infirm, not the young and healthy.
Measures can be adopted to protect the vulnerable without damaging or disrupting the lives of everyone else.
Natural immunity is robust and enduring, and when acquired in community settings, it expedites herd immunity and reduces the risks to the vulnerable.
Herd immunity is not dependent on vaccination, even if vaccination proves helpful.
The GBD marked a proverbial fork in the road for policymakers because it offered a high-profile off-ramp to extricate themselves from their injurious lockdown strategy. They could have used it as a platform to return to sound public health principles and messaging; tempering the excessive fears they had fostered by striking a more reassuring tone, while limiting further economic and social damage. From a political and public relations perspective, it provided cover to save face, and more importantly, to save lives.
“Canadians have developed a fear of COVID-19. Going forward, they have to be supported in understanding their true level of risk, and learning how to deal with this disease, while getting on with their lives – back to work, back to school, and back to healthy lives and vibrant, active communities across this country.”
Alas, as lawfully obtained emails revealed in December 2021, when the GBD was presented to covid’s most influential policymaker, Dr. Anthony Fauci, he balked at it. Rather than openly consider this sensible approach or engage in dialogue with its advocates, he doubled down on unproven restrictions. Worse yet, the emails revealed how Fauci and colleague Dr. Francis Collins colluded with media to discredit the GBD, intentionally stifling public debate about its merits. The fawning media’s adulation for Fauci has deterred most from critically examining his actions, but is it so inconceivable that a man with the audacity to proclaim “attacks on me, quite frankly, are attacks on science,” might be lacking for humility? Is it not disingenuous for him to declare “I represent science,” and then fail to recall any scientific justification for his covid directives when questioned about them under oath? If pressure reveals character, then what do these statements say about Fauci’s self-interest, diplomacy, and judgment?
It's hard to imagine a valid reason for social media – our digital public squares – to have prevented scientific discourse and discredited differing points of view during a period of uncertainty unless they felt pressured to do so. Why else would Google and Facebook censor the GBD and other exploratory covid content? Why else would Twitter blacklist credentialed and experienced professionals like the GBD authors? The answer arrived in January 2023, and it confirmed the worst fears of critics. The Wall Street Journal revealed that the White House’s director of digital media, Rob Flaherty, coerced social media giants into censoring posts that opposed the party line in an overt attempt to create the false impression of scientific consensus. In other words, science was poisoned by politics, which prioritized herd mentality over herd immunity. And this is the heart of the issue with censorship. It is incompatible with democratic values because it prevents conscientious dissent and the intellectual exercise of questioning beliefs, while presuming that authorities are unimpeachable arbiters of truth.
Censorship protects nobody while obstructing the only honest corrective mechanism in the marketplace of ideas – free speech. Free speech is the pathway to truth because it has an unlimited capacity for criticism and deliberation, which is the optimal filter for exposing the faults of bad ideas and illuminating the utility of good ones. Conversely, censorship selects arbitrary outcomes based on the pretense of knowledge, which are enforced by limiting the depth of information discovery and the breadth of debate. Although some naively argue that free speech is dangerous because it permits exposure to objectionable ideas, the alternative may authorize their unchecked proliferation, and that is a far greater evil. As it relates to covid, the damage from suppressing dissenting viewpoints continues becoming more apparent the more time passes.
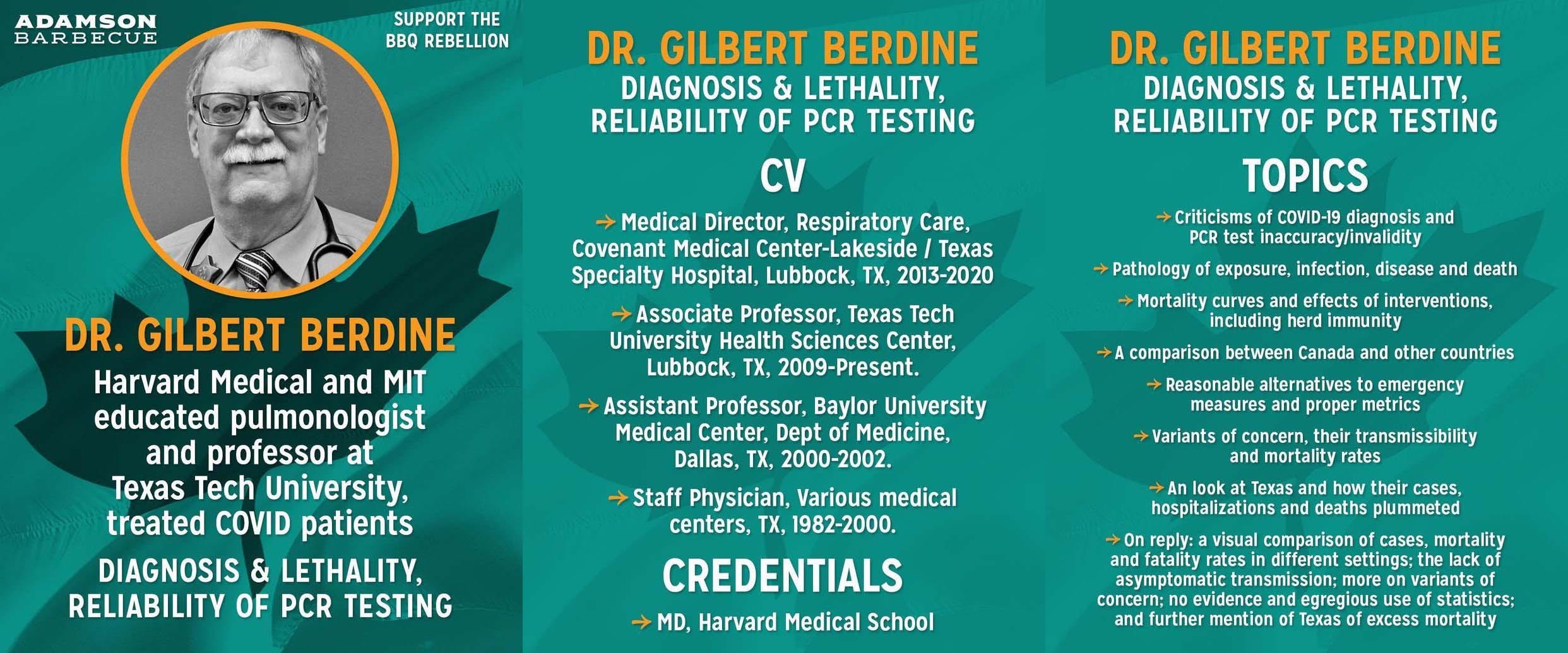
In testimony provided by Dr. Gilbert Berdine, a Harvard and MIT educated pulmonologist and Texas Tech professor, he argued that “Canadian lockdowns resulted in more deaths from COVID-19 than would have occurred by doing nothing.” His claim is supported by a rigorous data analysis of mortality rates stratified by age for different jurisdictions with different restrictions. It is further substantiated by the real-world outcome of countries like Sweden, which refrained from lockdowns, yet managed to maintain one of the lowest death rates among all Western countries according to both the WHO and the Organization for Economic Co-operation and Development throughout the covid era. According to lockdown proponents, roughly 3% of Swedes should have died – but they didn’t. Why not? As Warren Buffet famously said, “it's only when the tide goes out that you learn who has been swimming naked.” In the context of covid, the pierced veil of censorship has exposed that the emperors of lockdown have no clothes.
“We, or the Swedish government, decided early, in January, that the measures we should take against the pandemic should be evidence-based. And when you start looking around at the measures being taken now by different countries, you'll find that very few of them have a shred of evidence.”
– Johan Giesecke, Former Head Epidemiologist of Sweden. April 17, 2020.
PCR Testing & Case Counts
On the topic of testing, Dr. Berdine provided a critique of polymerase chain reaction (PCR) tests, the so-called ‘gold standard’ for detecting covid. He said that “there is no specific symptom, sign, or laboratory test for COVID-19. There is no way to be certain that a patient has a diagnosis of COVID-19… Published figures for sensitivity and specificity of PCR testing for COVID-19 are guesses based on presumed true positives,” and because of this “the obsession over cases is misguided.”
Explaining why this was the case, in August 2020, Dr. Robert Brown, Professor Emeritus at the University of Waterloo, wrote that “RT-PCR testing has been in use since the detection of the A (H5N1) influenza virus in 2005, but a serious limitation of RT-PCR testing is that nucleic acid detection is not capable of determining the difference between infective and noninfective viruses.”This was affirmed in a December 2022 study in the prominent science journal Nature, which mentioned that “no point-of-care diagnostic test currently exists to determine infectious SARS-CoV-2 in a patient sample.” Prior to covid, this had long been the position of the device’s Nobel Prize winning creator, Dr. Kary Mullis. Years ago, he explained how PCR tests “can find almost anything in anybody” because repeated amplification of samples increases the visibility of viral debris that are incapable of infection or transmission. Even if they could separate disease from debris, in August 2020, The New York Times acknowledged the inadequacy of the PCR testing regime, explaining how commonly used cycle thresholds were too sensitive and resulted in too many false positives to be a useful indicator. The article also addressed the economic and temporal disadvantages of PCR tests, but that’s a separate matter.
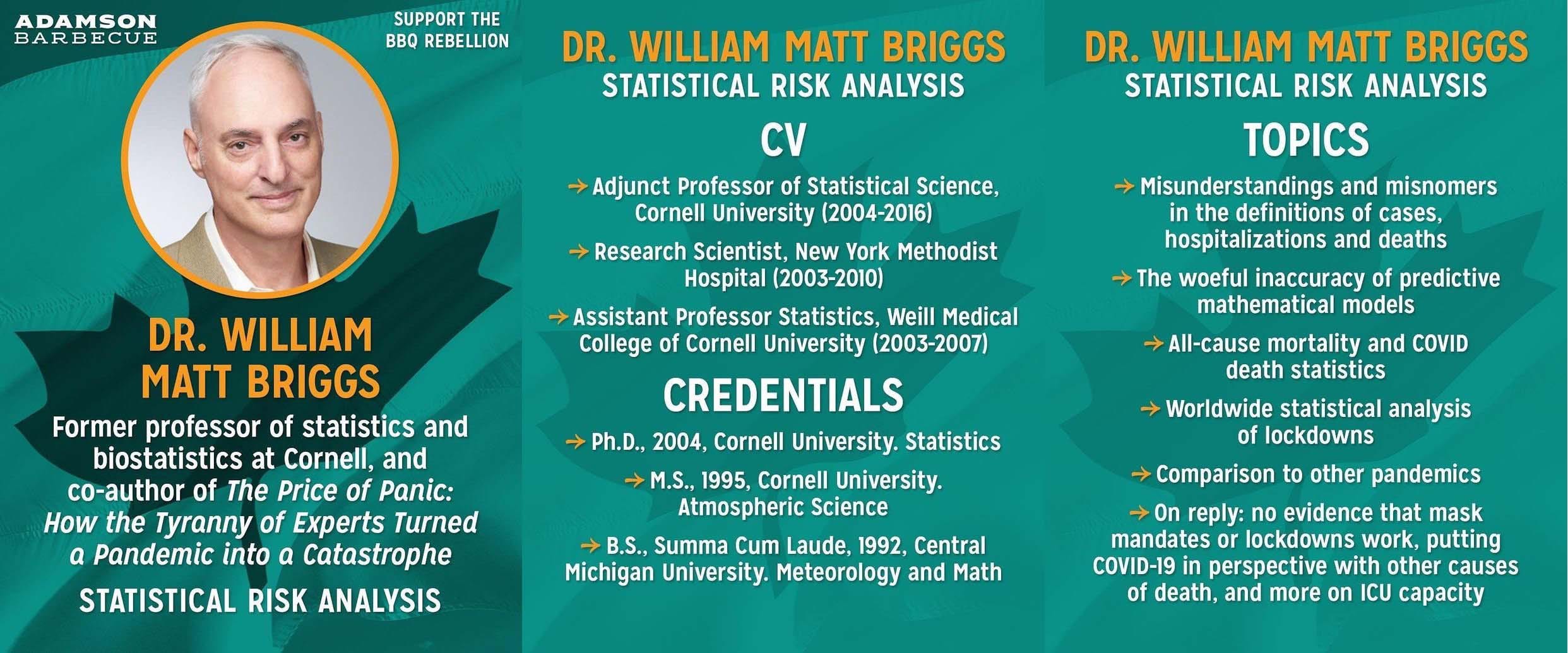
Testimony by another witness, Dr. William M. Briggs, a former professor of statistics and biostatistics at Cornell, said the implication of widespread PCR testing is that it “turns up marginal, slight, and asymptomatic infections, as well as false positives. Therefore, increased testing can give the impression the course of the disease is worse than it is.” Officials in Ontario confirmed this in July 2020, when the province’s Associate Chief Medical Officer of Health, Dr. Barbara Yaffe, explained that “if you’re testing in a population that doesn’t have very much covid, you’ll get false positives almost half the time… it will just complicate the picture.” Shortly thereafter, in October 2020, multiple Ontario public health units admitted to exaggerating covid death figures by including people who did not actually die of covid in their official totals, but it wasn’t until March 2022 when the province revealed that as many as 40% of deaths were wrongfully attributed. Importantly, in January 2022, Dr. Kieran Moore, Ontario’s Chief Medical Officer of Health, confessed that 45% of hospitalizations previously attributed to covid were not actually caused by covid, but were just incidental positive tests.
These admissions raise pertinent questions. If PCR tests were known not to be able to differentiate between infectious and non-infectious particles, why were results relied upon to inform policy? If it was known that PCR tests were unable to deliver accurate and timely data for the sake of tracking and tracing, why did public health continue reporting case counts? Additionally, if the role of media in democracy is to challenge official narratives, data, and methodology, to ensure transparency and accountability for the public, then why did they continuously broadcast “the numbers” without scrutiny or context? The alarming implication is that public health foolishly followed a misleading indicator, and our complicit media dutifully disseminated it, spreading misinformation that caused an anxious public to lose sleep, when they should have been counting sheep.
“Governments now propose that we test and trace all contacts of identified cases of disease. As we embark on this stage, we will find cases that would previously have gone unnoticed. Ironically, the better our testing capacity and the more we look, the more we will find, making it appear that disease is worsening, when it isn’t.”
– Doctors Neil Rau, Susan Richardson, Martha Fulford and Dominik Mertz. May 21, 2020.

Viral Transmission
Dr. Briggs also testified to the (lack of) statistical credibility supporting other tactics, such as case modelling, which not only influenced policymaking, but public perception. Even if we pretended that case counts were a meaningful metric, public health’s projections consistently missed the mark, and at day’s end all they accomplished was fomenting fear about worst-case scenarios. For example, the January 2021 model issued by the Public Health Agency of Canada (PHAC) predicted the country would surpass 10,000 daily cases by the end of February unless more restrictions were added. However, with no further restrictions added, cases fell below 3,000 per day by the end of February, proving their model wrong. Perhaps their forecasts were so far off base because they misunderstood covid how spreads?
This is not as far-fetched as it sounds. Initially, public health believed that covid lived on surfaces for hours on end, prompting many to disinfect everything from clothing to doorknobs to groceries. However, it turned out transmission via surfaces is exceedingly rare, if it even exists at all. Likewise, public health relentlessly touted social distancing, prompting many to avoid even the most marginal of encounters, but that also turned out to be ill-advised. There was never any basis for the six feet rule, which was an arbitrary distance chosen based on the false assumption that covid spread primarily through droplets. However, the predominant means of covid transmission was always aerosols, which remain airborne for hours, unlike droplets. Sadly, that’s not all they got wrong.
Remember how public health was originally overwhelmed with concern about asymptomatic spread, the novel notion that people who were not visibly sick with symptoms such as a cough, runny nose, or fever, could be contagious? Remember how it was used to rationalize quarantining millions of healthy people all over the world, constricting them into small bubbles, separating family and friends, closing businesses and activities, and shaming anyone who dared to hug grandma? It turns out those fears were also unfounded.
On June 8, 2020, the WHO’s technical lead for covid, Dr. Maria Van Kerkhove, acknowledged that asymptomatic spread was “very rare,” implying that covid behaved like any other coronavirus. This positive development should have been a relief, but strangely, it stirred outrage among influential physicians and pundits. Increasingly intolerant of information that lessened the threat, they pressured the WHO to walk back that remark the very next day. Nonetheless, the cat was out of the bag: health was not indefinitely out of reach, and disease was not an omnipresent threat. On November 20, 2020, an enormous study of millions of people in Nature found asymptomatic spread to be near non-existent. And in December 2020, a meta-analysis of 54 studies published in the Journal of the American Medical Association laid the misconception to rest for good. Referencing this analysis, Dr. Briggs concluded, “even inside households where person-to-person contact was inevitable, asymptomatic transmission was estimated at only 0.7%. This number could only drop outside homes.”
It was always suspicious that, according to the official narrative, covid continually defied all previously known means of viral transmission and intuitively dodged all countermeasures, even when they varied by jurisdiction. Every mask, every quarantine, every capacity limit, every plexiglass barrier, every missed activity, every curfew, every “non-essential” business closure, every color-coded restriction level – none of it was never enough to subdue the wily virus, even though regions that were less militant were less negatively affected. Going forward, if the public will to challenge authority and critically re-evaluate questionable premises like asymptomatic spread remains weak, then cognitive dissonance will stay strong, and those disseminating scientific fictions will be emboldened. Consequently, today’s deceptions may form the basis of tomorrow’s truths, especially in the minds of the young and impressionable, who will invariably build their future on those faulty foundations. If history is any guide, this too, is not as far-fetched as it sounds.
“Even if there is some asymptomatic transmission, in all the history of respiratory born viruses of any type, asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is always a symptomatic person. Even if there’s a rare asymptomatic person that might transmit, an epidemic is not driven by asymptomatic carriers.”
– Dr. Anthony Fauci, Coronavirus News Conference at White House. January 28, 2020.

Masks
With covid being aerosolized and asymptomatic spread being negligible, the argument for mask mandates rests on thin ice. To be clear, masks can be useful for sick individuals to contain droplets emitted from coughs, but that’s a one-way street preventing the sick from infecting the healthy, and the sick can still protect others by taking personal responsibility – as they have always done – by coughing into their arm, staying home, washing their hands, and treating their symptoms. High-quality, properly fitted masks have their uses in specific settings for short intervals, but their long-term use at the population level is highly problematic.
The hygiene hypothesis reminds us that extended withdrawal from the microbial world and natural environment can be harmful. Fresh air is crucial to our immune system development, and fresh faces are crucial to the human experience. On December 15, 2022, Dr. Moore re-discovered this formerly common knowledge, stating, “we are obviously seeing that there are some negative consequences to not being exposed to the normal respiratory pathogens over time.” This, it would seem, was an understatement.
“The bottom line is there is no solid scientific evidence to support cloth face masks. Unless they’re medical-grade, they will do no more than catch large expectorated secretions from people who should be staying home if they’re hacking and coughing.”
– Dr. David Colby, Former Medical Officer of Health for Chatham-Kent. August 6, 2020.
At present, there are hundreds of studies documenting the ineffectiveness and harms of widespread mask use. Socially, masks plainly prohibit facial expression, which as the still-face experiment of 1978 long ago proved, facial cues are crucial for emotional development. Drawing attention to the potential disadvantages of masks, SickKids Hospital acknowledged in July 2020 that, “facial expression is a critical part of communication,” and that masks may “adversely impact education and interaction, particularly non-verbal communication skills.” As it relates to healthcare, the 2006 Ontario’s SARS Commission report explained that N95 respirator masks “restricted human interaction (an important part of patient care).” In that same report, the Ontario Nurses Association (ONA) and Ontario Public Service Employee Union (OPSEU) described some of the physical drawbacks of N95 respirators. They told the Commission that health workers experienced a slew of issues from prolonged usage, such as throat irritation, headaches, upper chest tightness, dizziness, oxygen deprivation, and increased carbon dioxide intake. As for regular surgical masks, the Commission itself wrote, “studies have shown that surgical masks, because of their inability to create a tight seal, are less effective against smaller droplets and droplet nuclei than N95 respirators. Even wearing as many as five surgical masks does not raise their ability to filter out smaller airborne particles.”
Making matters worse, masks themselves are not assured to be sanitary. For example, in December 2020, 31.1 million masks distributed to 15,000 daycares in Quebec failed their safety checks, but only after they had been worn for months. Shortly thereafter, in March 2021, the province recalled another set of masks, this time because they were coated in graphene oxide – a toxic substance linked to lung disease and cancer. Those masks were also distributed to millions by the government and worn by unsuspecting adults and children. And even if masks were sanitary to begin with, proper hygiene practices must be used to avoid contamination. As it is, the inside of a mask is a warm, moist environment conducive to bacterial growth. It can get saturated in as little as 15 to 20 minutes. Just imagine the damage that can be done over 15 to 20 months of persistent, improper use.
This drawback has long been understood by trained professionals as a legitimate health risk, but if further confirmation were necessary, in June 2021, a lab analysis of children’s masks after a day of school discovered that they were contaminated with bacteria, parasites, and fungi, including some with dangerous pathogenic and pneumonia-causing bacteria. Regrettably, health officials wholly ignored these well-known costs during covid, discounting the value of fresh air and smiling faces to zero.
“The trouble with ordinary surgical masks are you lick them and you stick your nose in them and they have big holes in the outside part and so forth. Let’s face it, they’re a joke.”
– Testimony to SARS Commission by unnamed Toronto physician that treated SARS patients. December 2006.
In preventing the transmission of covid, the real-world benefits of universal masking have proven trivial. The two most cited randomized control trials (RCT) – the highest quality form of scientific evidence – indicated that masking had a marginal impact at best. First, the DANMASK trial from March 2021 showed masks had virtually zero effect in preventing individuals from catching covid when worn in public. The trial was criticized because it evaluated masking at a personal level, not community level. However, another RCT, the Bangladesh mask study from December 2021, showed that, with very few exceptions, masks had little to no effect on the community spread of covid. More recently, in January 2023, a massive study by the Cochrane Review consolidated data from multiple RCT’s and, once again, the results “did not show a clear reduction in respiratory viral infection with the use of medical/surgical masks.” To quote the study’s authors, “wearing masks in the community probably makes little or no difference to the outcome of influenza‐like or COVID‐19-like illness transmission.” Poetically, they also added, “We failed to follow an evidence-based approach during the pandemic. We are now left with the human, social and economic aftermath of evidence-free policies.”
None of this should come as a surprise to the ONA, which has long known that the utility of masking is limited. In 2015, the ONA actively fought against mandatory masking when roughly 30 hospitals in Ontario attempted to implement a ‘mask or vaccinate’ policy for the seasonal flu. They decried the hospitals for “coercing and shaming nurses into getting the influenza vaccine if they individually chose not to take it.” The ONA also fought the policy on the grounds that “they are outing you, because your personal health information – whether you get vaccinated or not – is now public knowledge.” Their case relied on experts who testified on the logical inconsistency of having healthy nurses wear masks, and the arbitrator agreed, concluding that masks were not protecting patients or nurses, and that the policy was unreasonable because it was coercive. The ONA president at the time said the policy was “symbolic rather than scientifically based,” and amounted to a “draconian shaking of finger at nurses.” Similarly, in December 2019, the British Columbia Nurses Union (BCNU) celebrated a new agreement with the province’s Health Employers Association, which the BCNU president said ensured “the professional judgment of nurses is respected,” by ending the “punitive nature” of their ‘mask or vaccinate’ policy. Reading these statements, irony abounds, as yesterday’s defenders of workers’ rights sound an awful lot like today’s so-called “misinformation spreaders.”
Considering that the ‘experts’ did an about-face on face coverings and that industry associations across the country failed to fight for members’ rights to bodily autonomy and medical privacy, is it really any wonder why mask mandates were vociferously challenged over the last few years? In the right place, for the right reason, for a limited time, and worn by the right person, a mask might make sense. As a blanket measure for the public – they are suffocating. The futility of universal masking should have been acknowledged long ago, if only logically inconsistent ‘experts’ hadn’t duped themselves into believing their own masquerade, becoming unironically intoxicated by it.
“Little evidence exists as to how effectively the wearing of a mask by well individuals will prevent them from becoming infected… If not used properly, masks may lead to a greater risk of pandemic influenza transmission because of contamination… wearing them for prolonged periods may be impractical and ineffective. It is important to present the limitations of mask use to the public.”

Mortality Rates
Any remaining reluctance to relinquish masks likely stems from a misunderstanding of covid’s mortality dynamics. It has long been known that covid primarily afflicts the elderly and infirm, but this fact was largely omitted from the national conversation that shaped covid policies. Drowned out by the anxiety-inducing noise of press briefings, case count updates, on-the-fly rule changes, slogans like “stay home, save lives,” and more, many missed the sensible signal broadcast by compassionate doctors and health advocates. They published numerous op-eds in the media describing the age stratification of covid and the prolonged suffering caused by restrictions, but time and again, their warnings fell on deaf ears.
In May 2020, a group of infectious disease experts wrote that “95 per cent of COVID-19 deaths occurred in those over 60, compared with none under age 20. Protection of the former group deserves the most attention; this will be easier if limited resources are diverted from other, low-risk groups.” In July 2020, a large group of current and former health leaders penned an open letter, which explained that “in overall population health terms COVID-19’s direct impact on premature mortality is small. While those under the age of 60 account for 65% of cases, they represent just 3% of deaths.” They also added that “the societal costs of maintaining these public health measures, even with some gradual relaxation, are too high.” In October 2020, a group of physician mothers literally pleaded for mercy from authorities on behalf of our youth, saying “it is with increasing distress that we have watched Canadian decision-makers de-prioritize the legitimate needs of our youth… the risk of dying of COVID for the young is hundreds of times less than dying of other things… the medical and statistical truth is that the young are not at risk from COVID-19.”
“For children without a serious medical condition, the danger of severe Covid is so low as to be difficult to quantify.”
– David Leonhardt. Senior Writer at The New York Times. October 12, 2021.
All their claims are backed up by official public health data. A StatsCan update on mortality covering the period of January 2020 to April 2021 documented a notable rise in excess deaths among those under age 65, which implied they were four times more likely to die due to restrictions than covid. In October 2021, the Public Health Agency of Canada published a fact sheet explaining that “the majority of COVID-19 deaths (approximately 80% during 2020) occurred among adults aged 65 years and older. Both advanced age and underlying chronic diseases and conditions contribute to these severe outcomes.” And as per the December 2022 Government of Canada epidemiology update, of the near 49,000 deaths attributed to covid throughout the country, 93% occurred in those over age 60, with 82.4% being over 70. Conversely, only 1.2% of deaths occurred in those under 40.
In December 2022, an extensive analysis by the world’s most credentialed and cited epidemiologist, Stanford’s Dr. John Ioannidis, not only re-confirmed age and comorbidity as determining factors of covid severity, but also that “the absolute number of fatalities are overall probably modestly higher than seasonal flu fatalities over three typical pre-pandemic years.” Astonishingly, the assessment that covid amounts to no more than a bad flu was initially shared by none other than Dr. Fauci, who published a study in the New England Journal of Medicine (NEJM) on March 26, 2020, where he predicted that, “if one assumes that the number of asymptomatic or minimally symptomatic cases is several times as high as the number of reported cases… the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%).” If Fauci had followed his own research, a lot of pain and suffering could have been avoided.
Despite ample evidence suggesting covid was a molehill, those entrusted to keep the public informed remained adamant it was a mountain. They failed to admit their mistakes or consider a second opinion, even when there was material proof that the severity of the disease was significantly overstated. What does that say about their integrity? What does that say about their leadership qualities? What does that say about their scientific acumen? Shamefully, health pundits and politicians continue clinging to their misguided narrative three years into this mess, proving that their misrepresentation of covid’s mortality is no mere misunderstanding, but a monumental breach of public trust. The implications of this are as serious as a heart attack because trust, once lost, is not easily regained.
“We just got lucky that the death rate per case was like 0.2%... we didn’t understand it’s a fairly low fatality rate and that it’s a disease mainly in the elderly, kind of like the flu, although a bit different.”
The Healthcare System
There is one more angle to the mortality issue that warrants exploration. In Dr. Briggs testimony, he referenced the March 2021 statistics from the Government of Canada epidemiology update page, noting that “there is a breakdown of where covid deaths are found… the majority, or just under 92% (12,372 in total), were recorded in long term care and retirement residences. The next largest, at 6%, was in healthcare.” Including prisons, 98.6% of covid deaths occurred in just three settings. And what do those settings have in common? As astute covid policy critic and data analyst Julius Ruechel commented, those are “captive populations that are permanently or semi-permanently segregated from the rest of society inside government-owned or government-regulated institutions.”
Traditionally Canadians have revered their healthcare institutions, but is that faith still justified? Long before covid, Canada’s healthcare capacity had been faltering. According to data from the World Bank, Canada had 6.8 hospital beds per 1,000 Canadians in 1980, declining to 6.0 in 1990, before falling off a cliff thereafter. By 2005, there were only 3.1 per 1,000 Canadians, and as of 2019, there were only 2.5. Current Organization for Economic Co-operation and Development (OECD) data has Canada with the 6th lowest rate of hospital beds per capita out of 37 ranked countries, and the 4th lowest rate of intensive care beds out of 34 ranked countries. What happened? How is it that, over the course of 40 years, both left- and right-wing governments failed to build out or even maintain hospital capacity, especially given Canada’s aging population and high immigration?
It's not as if politicians weren’t aware of the issue – it’s been front and centre for decades. In 2000, the New York Times wrote about Canadians looking for healthcare in the US due to full hospitals. In 2002, Prime Minister Jean Chrétien’s brother was left in a hospital hallway due to overcrowding issues. In 2005, SickKids hospital was stretched thin to the point of running out of intensive care beds, with viral season said to have played a role in the burden. In 2008, the Toronto Star reported on backed up emergency rooms leading to hallway medicine. In 2010, hospital overcrowding was dubbed Ottawa’s biggest local health story of year. In 2011, the Globe & Mail reported how a surge of flu cases were overwhelming hospitals. In 2013, hospitals were again reported as being overwhelmed by the flu. In 2015, yet more reports of hallway medicine and bed shortages. In 2016, a Globe & Mail report highlighted hospitals operating beyond their capacity. In 2017, hospitals were again running out of space. In 2018, overcrowding caused patients to receive “substandard” care across Ontario, leading to increased infections and postponed surgeries. In 2019, the Ontario Hospital Association reported that hospital bed capacity had not increased over two decades despite a 27% population increase. Finally, in January of 2020, just before covid, CBC News discovered dozens of hospitals operating over capacity.
If any of these headlines sound familiar, it’s because many were essentially recycled over the last few years with a spikey new scapegoat, putting into perspective how blaming covid – or for that matter, the unvaccinated – for hospital capacity woes was like blaming the rain because you didn’t buy an umbrella. It’s disingenuous, and it deflects from the bigger picture. The healthcare system is not a wedge to be weaponized against those who fund it. It is a service into which all Canadians pay explicitly for its universal availability. If it is unable to fulfill its obligations, then funding ought to be withdrawn and invested into new systems, or the existing system must address its deficiencies and restructure accordingly. Once again, Ruechel said it best, “[covid] is not a general population crisis; it is an institutional crisis.”
“Overcrowding has become so common in Ontario hospitals that patient beds are now placed in hallways and conference rooms not only at times of peak demand, but routinely day after day… hospital gridlock – a phenomenon that used to be restricted to surges in patients during flu season – is the new normal.”
– Mike Crawley, Senior Reporter, CBC News. January 22, 2020.
There are those who blame the healthcare system’s deficiencies on spending shortfalls, but that oversimplifies the issue. Funding has ebbed and flowed over the last few decades, but in general, Canada’s healthcare spending is in line with many comparable countries. So, why does it typically generate a lower return on investment than its peers? No doubt it would help if the healthcare establishment trimmed some fat, reducing its excessive ratio of administrators-to-doctors, whose paper-pushing requirements divert doctors’ time away from caring for patients. According to the Canadian Federation of Independent Business (CFIB), Canadian doctors spend 18.5 million hours per year doing unnecessary paperwork – that’s the equivalent of 55 million patient visits. Additionally, the healthcare system actively prevents qualified doctors from entering practice. A February 2023 report by CBC News explained how the current residency system is constrained by red tape. It excludes Canadian doctors who train abroad, has a poor placement rate, and has unnecessary vacancies, such as the 115 residencies (mostly in family medicine) that went unfilled last year. All told, Canada’s bloated healthcare bureaucracy yields diminishing returns, drives up costs, and inefficiently allocates scarce resources, stifling capacity and generating backlogs. But those are merely symptoms of the problem. The root cause is an institutional culture at odds with accountability and foresight – and covid put a spotlight on all of it.
In 2020, frontline healthcare staff were hailed as heroes, returning home each night to a chorus of clanging pots and pans. Availing themselves of their newfound popularity, some took to TikTok, supposedly making dance videos to blow off steam. However, a study in the American Journal of Nursing analyzed those videos and determined that many were inappropriate, violating various codes of conduct, including ethics provisions, social networking principles, and social media guidelines. This raises an interesting question – was covid a valid excuse to abandon professionalism? If anything, shouldn’t it have been a reason to renew commitment to, and abide by, professional standards? Moreover, did it not occur to staff and administrators that using personal protective equipment (PPE) as props, which have been in short supply for decades, might send the wrong message to the public, downplaying the purported seriousness of covid and exhaustion of staff?
In 2021, Ontario spent tens of millions of dollars erecting field hospitals that were seldom used, including one in Hamilton with a capacity of 80 patients that had zero visitors throughout its lifecycle. Wouldn’t that money have been better spent on long term capacity or staffing, both of which are always in need? Later that year, healthcare staff who did not bend the knee to vaccine supremacy were forced out of their jobs – experience, immunity, and valor be damned. Did hospital administrators not realize that tossing out qualified staff like yesterday’s trash might exacerbate existing shortages? Did it not occur to them that unilaterally claiming jurisdiction over workers’ bodies and cancelling employment insurance benefits might set a bad precedent, causing prospective employees to think twice before working for them in the future? Then there is the College of Physicians and Surgeons of Ontario (CPSO), which issued a statement prohibiting doctors from speaking out against lockdowns, masks, and other issues that did not conform to public health groupthink. Did the college honestly believe it was sound policy to muzzle doctors from speaking out against the harms they witnessed inflicted on their patients? Did the college not understand that this sort of intellectual immaturity would undermine their credibility?
“I get very uncomfortable with people being fired over this… There’s not much of a spirit of understanding at all… Our goal as health-care works is to make sure that our patients… are making informed decisions… This has shifted to: do we like your decision or not?"
– Dr. Kerry Bowman, Bioethicist, interviewed on CBC’s Cross Country Checkup. October 17, 2021.
Circling back to how all this affects long-term care and retirement homes – where 92% of covid deaths occurred – consider how these government-regulated institutions treated society’s most vulnerable. As with hospital capacity, Ontario’s Minister of Long-Term Care acknowledged that these facilities have been neglected for decades. The increased burden from covid measures were merely the straw that broke the camel’s back. In a May 2020 report by the Canadian Armed Forces (CAF), which were called to assist at a number of these facilities in Ontario in April 2020, they described the conditions there as “heartbreaking,” “horrifying,” and “in a general state of disrepair.” Facilities were infested with cockroaches, fungus, and mould. Vomit and feces were found on floors and walls. The CAF suspected many residents died from neglect and malnutrition, even though covid was blamed.
Similar circumstances were also uncovered in Quebec, where according to the Globe & Mail, a “lack of humanity [was] afforded to dying residents.” At the Quebec Coroner’s Inquest, one nurse said “I had the impression that they were blaming the virus because it would be easier to blame the virus than to acknowledge the hard truth that these people suffered from malnourishment and dehydration. I felt that it was a way to escape culpability.” Once again, deaths attributed to covid in official statistics were more likely the result of onerous restrictions, which expedited residents’ decline by preventing contact with loved ones and interfering with nurses’ ability to provide timely medication, sanitation, and sustenance. Worse yet, some staff abandoned their posts entirely even when there was nobody to replace them, but thankfully many brave staff continued caring for patients despite the unforgiving circumstances.
In the end, the healthcare system that authorities said required saving via sacrifice from millions of healthy Canadians failed miserably in its objective, abandoning those who most relied on it in their most desperate hours of need – and then the system crumbled anyway. What does that say about those making and enforcing healthcare policies? What does it say about those who follow them without question or resistance? What does it say about those who control its purse strings? To whom is the healthcare system and its practitioners ultimately accountable – rent seeking administrators or taxpaying patients? Failing a dramatic change of priorities, no amount of money can fix what’s broken.
“SARS showed Ontario’s central public health system to be unprepared, fragmented, poorly led, uncoordinated, inadequately resourced, professionally impoverished, and generally incapable of discharging its mandate.”
– The Honourable Mr. Justice Archie Campbell, Ontario SARS Commission, Interim Report. April 15, 2004.

The Pharmaceutical Industry
Politicians, associations, colleges, and administrators are not the only ones that need to check their priorities. In 1994, the nation’s health regulator, Health Canada, introduced a user fee funding model that brought on pharmaceutical companies as partners to finance key aspects of drug regulation. In effect, they invited the fox to guard the henhouse. Although regulators and pharmaceuticals have always had a cozy relationship, this development consummated their union. As it stands today, 90% of funding for drug regulation comes from the pharmaceutical industry. The problem with this is the obvious conflict of interest arising from the principal-agent relationship, whereby Health Canada’s concern for public safety and the pharmaceutical industry’s profit motive are not always compatible. As a result, this model has been the subject of ongoing and justifiable criticism, especially given its shifting priorities. Since this arrangement took effect:
New drug application funding and staffing increased three to four times, whereas product safety monitoring received no additional resources. This increased the difficulty of monitoring, reviewing, and recalling previously approved drugs, because more drugs make it to market, and there are comparatively fewer resources for their necessary, continual evaluation.
Safety and efficacy data from industry-run clinical trials can be withheld from the public. Abetted by Health Canada, the pharmaceutical industry makes legal claims of “trade secrets” and “confidential business information” to protect their data, but this reduces transparency for substances of public interest, keeping doctors in the dark about relevant information that can – and has – put patients at increased risk.
The regulatory process for drug approvals has been sped up. Where there are shorter approval times, more serious safety concerns tend to follow, and between 1995 and 2010, nearly 24% of approved drugs were later found to have serious safety issues.
Unfortunately, the medical journals are also compromised by the pharmaceutical lobby. In 2004, the editor of leading journal The Lancet, Richard Horton, wrote that “journals have devolved into information laundering operations for the pharmaceutical industry,” which employ various strategies to boost positive results and suppress negative ones. In 2005, the former editor of the British Medical Journal (BMJ), Richard Smith, wrote that “medical journals are an extension of the marketing arm of pharmaceutical companies.” Back in 2001, the editors of 13 general medical journals wrote a commentary in the Canadian Medical Association Journal decrying the changing incentives of medical research, which led to waning funding for independent researchers with reputations for intellectual rigor and honest hypothesis testing, while increasing funding for studies designed to target regulatory approval. The net effect of this is more drugs on the market and less critical review of their performance. Clearly, these trends are not in the public’s best interests. The last couple decades have seen a lot of ink spilled on this topic – to the point it’s basically an open secret that the integrity of medical journals has been debased – but consequential policy changes have not been forthcoming. And so long as the status quo remains, extra doses of “healthy” skepticism are recommended.
“Corporate sponsors have been able to dictate the terms of participation in the trials, terms that are not always in the best interests of academic investigators, the study participants, or the advancement of science generally. Investigators may have little or no input into trial design, no access to the raw data, and limited participation in data interpretation.”
– Editors of 13 General Medical Journals, Canadian Medical Association Journal. September 18, 2001.
Of further concern, doctors and medical schools are also enveloped by the pharmaceutical industry’s tentacles. Exposing this in detail, Global News released a bombshell four-part investigation on this topic in the summer of 2019. Part one explained how Purdue Pharma, the infamous creator of the wildly addictive opioid OxyContin, would wine and dine doctors, serenading them with “carefully honed” key messages to sway them into prescribing the product. Among those messages were that OxyContin was not addictive, that it was “safe and effective,” and that doctors were “opiate-phobic” if they had an “irrational” fear of opiates. Draw your own parallels to the terms “anti-vax” and “vaccine hesitancy.”
Part two of the series elaborated on drug representatives’ influence over physicians, explaining how drugs are aggressively promoted early in their lifecycle before concrete evidence of their safety and efficacy emerge. Why? Quoting from a BMJ study cited in the investigation, independent studies have shown that “85-90% of new products over the past 50 years have provided few benefits and considerable harms.” Additionally, new drugs are typically more expensive than older or “off-patent” drugs because prices of the former are artificially inflated via exclusive production rights, while prices of the latter are determined on the open market where producers compete to offer the best prices. For new drugs, this means there is a limited window of opportunity to cash-in before exclusivity expires and any deceptive data is exposed. Considering the meager cost-benefit profile of most new drugs, which needlessly burdens patients, drug plans, and taxpayers with excess costs, why should new drugs receive even the slightest benefit of the doubt? Shouldn’t the default position of doctors and regulators be to presume that pharmaceutical-sponsored trial data is incomplete or misleading? Why isn’t it a requirement for safety and efficacy to be proven by independent studies?
“Physicians don’t have access to the full data and the drug companies still choose what to publish. They don’t say anything about negative results… so the development of new products is about selective ignorance.”
On a related note, the investigation cited Adriane Fugh-Berman, the director of a project to advance evidence-based medicine at Georgetown University Medical Center called PharmedOut, who said the sad truth of the matter is “doctors think they can extract the good information from the bad, and they can’t. That’s been documented.” Echoing this sentiment, renowned Canadian emergency care physician, professor, and author, Dr. Joel Lexchin, told CTV Newsin a September 2017 interview that, “we know from studies in other countries that, even though doctors may not realize it, they can be influenced by payments they get from pharmaceutical companies.” He poignantly added that “some doctors might be concerned about this… and if you’re concerned about it then perhaps you should stop taking the money.”
To be clear, it’s not that doctors are sellouts who callously trade patient health for material wealth. Far from it. The majority are well-intentioned and care a great deal about their patients’ well-being, but they have grown too trusting of untrustworthy institutions, and too comfortable with the pharmaceutical industry’s influence. To that end, parts three and four of the investigation explained how doctors, medical schools, and hospitals, have difficulty maintaining their impartiality because pharmaceutical companies are constantly doling out spoons full of sugar to help their medicines go down. Part three explained how millions of dollars are funneled into medical schools by sponsoring textbooks, running courses and workshops, funding faculty research, and more. All of that normalizes relationships with drug representatives and affects the prescribing habits of doctors. Lastly, part four investigated payments and donations to hospitals and doctors, explaining how paid speeches, trial participation, advisory board membership, and travel expenses for conferences influence prescriptions, and also that Canada has weak transparency rules and institutional safeguards.
“[Purdue Pharma] dramatically changed physicians’ prescribing habits of opiates. The interesting thing is that these messages were false, and they knew them to be false at the time, and they didn’t care. And even when evidence emerged – which was pretty quickly – that people were dying of OxyContin overdoses, they still persisted.”
For their part, pharmaceutical companies are well-aware of their duplicitous tendencies, and shockingly unconcerned by them. Prescription drugs are among the leading causes of death in the US and Europe (Canada does not track this statistic), and that includes drugs taken in the correct doses. Additionally, medical errors are thought to be a significant cause of death in both Canada and the US. Flouting the law and flaunting their disregard for the devastation their products have caused, in January 2020 Dr. Joel Lexchin explained that some pharmaceutical companies even have “a position they euphemistically called vice-president in charge of going to jail.” This means that, if anything, penalties for bribing physicians, suppressing adverse trial results, and deceitful marketing – all of which are habitual practices for pharmaceutical giants like Pfizer – are merely business expenses to be weighed against revenues, similar to how the banking industry approaches fines for money laundering, market manipulation, and other violations. Presciently, Dr. Lexchin added that, “it all comes in cycles and the next disaster will be just as bad.” In other words, the pharmaceutical industry’s response to covid was perfectly predictable; it was a golden opportunity to push new products and generate record profits, regardless of patient safety.
From education to practice to regulation to research, the pharmaceuticals have the healthcare industry in a bearhug. Having compromised any institution that might push back against their corrupt practices, modern pharmaceuticals are no longer a means to an end – to health – but an end unto themselves, which uses the healthcare system as its means. And as a result of allowing itself to be dominated by the products it was meant to master, the healthcare industry has seemingly become disinterested and powerless to stop the veritable epidemic of harmful side effects caused by pharmaceuticals. It may be a tough pill to swallow, but all this implies that the slogans “follow the science” and “trust the experts” were misleading because they ignored the tragic truth that both ‘science’ and ‘experts’ are conspicuously manipulated by the pharmaceutical industry.
“Evidence suggests that commercial distortions of the review process and aggressive marketing contribute to both undermining beneficence as health care's raison d'être and to the epidemic of harm to patients.”
– Doctors Donald L. Wright, Joel Lexchin, and Jonathan J. Darrow. Journal of Law, Medicine & Ethics. Fall 2013.

Treatments & Immunity
With the advent of covid and the healthcare system on life support, it made sense that authorities would want to keep patients out of hospitals. Then again, it always makes sense for people to be healthy and avoid hospitals. To that end, a quality diet, active lifestyle, social connectiveness, and exposure to the natural world are all essential for a strong body, mind, and immune system. On occasions when medical interventions are necessary, early treatment is a crucial tool in any doctor’s toolbox. Treating sickness before it progresses to critical stages can alleviate the burden on under-performing healthcare institutions and lessen the duration of patient suffering.
In certain circumstances, doctors are permitted to prescribe “off-label” (not for original or intended purpose) medicines. Dealing with an unknown quantity such as covid surely should have qualified. For patients experiencing severe symptoms, responsibly administering readily available, cost-effective drugs with anti-viral properties and strong safety track records should have been a no-brainer. Even if efficacy was not well defined, the potential benefits as a countermeasure to covid – a novel coronavirus – clearly would have outweighed the risks.
One such candidate was hydroxychloroquine (HCQ), which gained prominence in March 2020 after then-President Donald Trump was prescribed the drug by his doctors to treat his case of covid. However, less than two weeks after the FDA granted HCQ Emergency Use Authorization (EUA), two former FDA commissioners complained that using it would hurt ongoing clinical trials; an illogical excuse that prioritized politics over lives and pre-emptively dismissed positive developments documented by renowned scientists. Just two months later, in June 2020, the FDA reversed course and revoked the EUA, claiming HCQ was unlikely to be effective and accusing it of having serious side effects. Regarding its efficacy against covid, the evidence may not yet have been conclusive, but it was undeniable that there were positive signs – that’s why it received emergency approval in the first place. As for safety, HCQ has been an FDA-approved drug since 1955. That’s a 68-year track record. It is so safe that the WHO includes HCQ on its List of Essential Medicines. For the FDA to suddenly suggest without strong evidence that HCQ had serious side effects seemed disingenuous, and it raised more questions than it did provide answers.
“I think that the FDA has learned nothing. The modus operandi of the agency is that they talk a good game and then nothing happens… The lack of insight that continues to be exhibited by the agency is in many ways a willful blindness that borders on the criminal.”
– Dr. Raeford Brown, Chair of the FDA’s Opioid Advisory Committee. January 24, 2019.
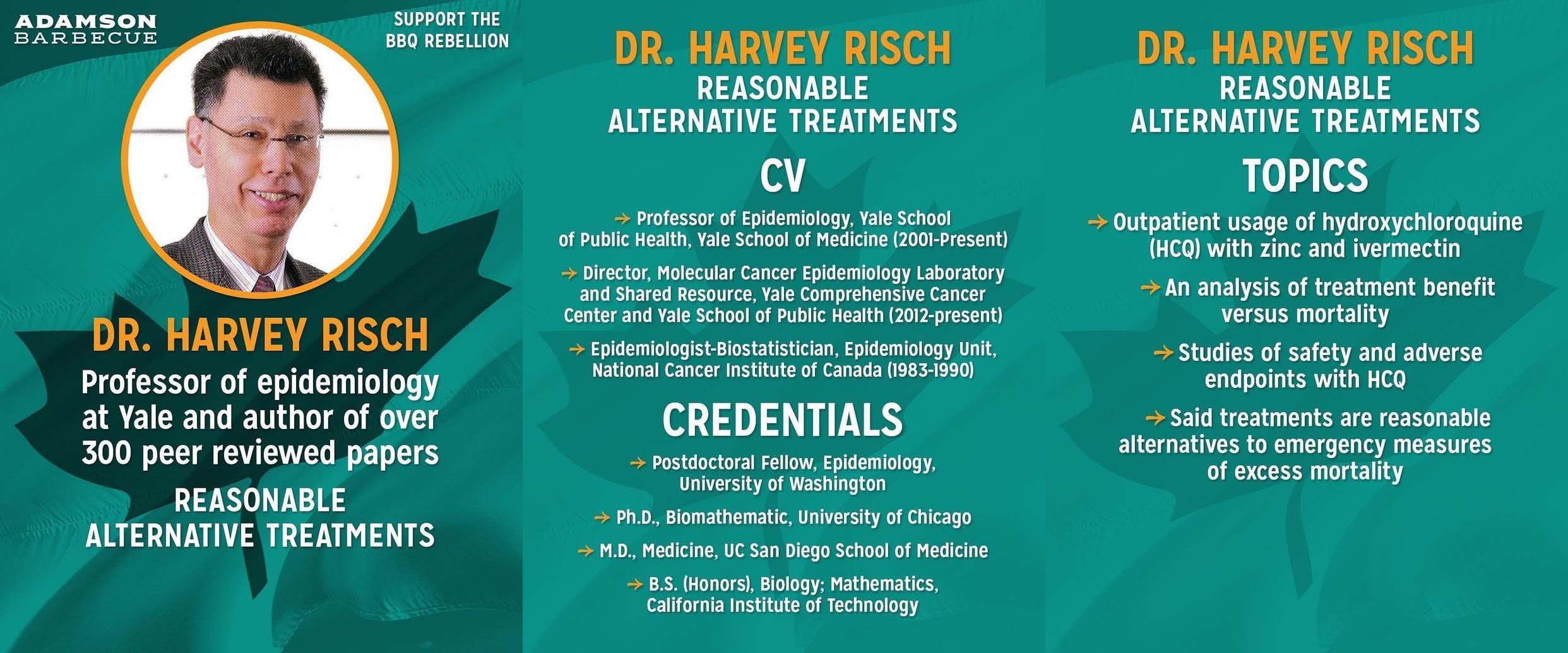
According to witness testimony submitted by Dr. Harvey Risch, professor of epidemiology at Yale University, when it comes to the safety of HCQ, “the FDA has no systematic evidence of fatal adverse events from hydroxychloroquine prophylaxis or outpatient treatment use and has invalidly used evidence in hospitalized inpatients to create a false public warning by extrapolating to outpatient use.” As for the FDA’s claims of inefficacy, he wrote that “the RCT studies proclaimed supposedly as definitively showing no benefit of HCQ use in outpatients have all involved almost entirely low-risk subjects with virtually no hospitalization or mortality events and are uninformative and irrelevant for bearing upon these risks according to HCQ use in high-risk outpatients.” Having accounted for this oversight, he stated that “it is readily apparent that every one of the studies of high-risk outpatient HCQ use has shown 2-fold or better risk reduction for hospitalization or mortality, and that the numerous systematic case-series studies have shown exceedingly good treatment benefit vs mortality.” Based on this, he concluded that “the improper warning on the FDA website must be removed immediately, and widespread early outpatient treatment must start immediately.” Given that, as of February 2023, a real-time tracker of HCQ results spanning 382 studies shows it consistently yielded positive outcomes when used as an early treatment, Dr. Risch’s allegations about the FDA’s erroneous conclusions warrant further investigation.
Even more polarizing than HCQ was ivermectin (IVM). Discovered in 1975 by Dr. Satoshi Omura and approved for human use in 1987, it was hailed has a miracle discovery for its incredible anti-parasitic properties. In 2011, Dr. Omura wrote, “there are few drugs that can seriously lay claim to the title of ‘Wonder drug’, penicillin and aspirin being two that have perhaps had greatest beneficial impact on the health and wellbeing of Mankind. But ivermectin can also be considered alongside those worthy contenders, based on its versatility, safety and the beneficial impact that it has had, and continues to have, worldwide.” This sentiment was echoed in a 2017 Nature study, which praised IVM’s versatility, saying “today, ivermectin remains a relatively unknown drug, although few, if any, other drugs can rival ivermectin for its beneficial impact on human health and welfare.” For discovering and developing IVM, Dr. Omura and Dr. William C. Campbell were awarded the Nobel Prize in medicine in 2015. It is also on the WHO’s List of Essential Medicines.
“Ivermectin is highly effective against a range of parasites, has limited side effects and is freely available across the globe… Treatment is so successful that these diseases are on the verge of eradication, which would be a major feat in the medical history of humankind… The global impact of their discoveries and the resulting benefit to mankind are immeasurable.”
What does an anti-parasitic ‘wonder drug’ have to do with covid? Among its many healing capabilities, IVM happens to have strong anti-viral properties. According to the same 2017 Nature study, “ivermectin has also been demonstrated to be a potent broad-spectrum specific inhibitor of importin α/β-mediated nuclear transport and demonstrates antiviral activity against several RNA viruses by blocking the nuclear trafficking of viral proteins.” The study also touted IVM’s noteworthy anti-bacterial and anti-cancer properties, but that’s another story altogether.
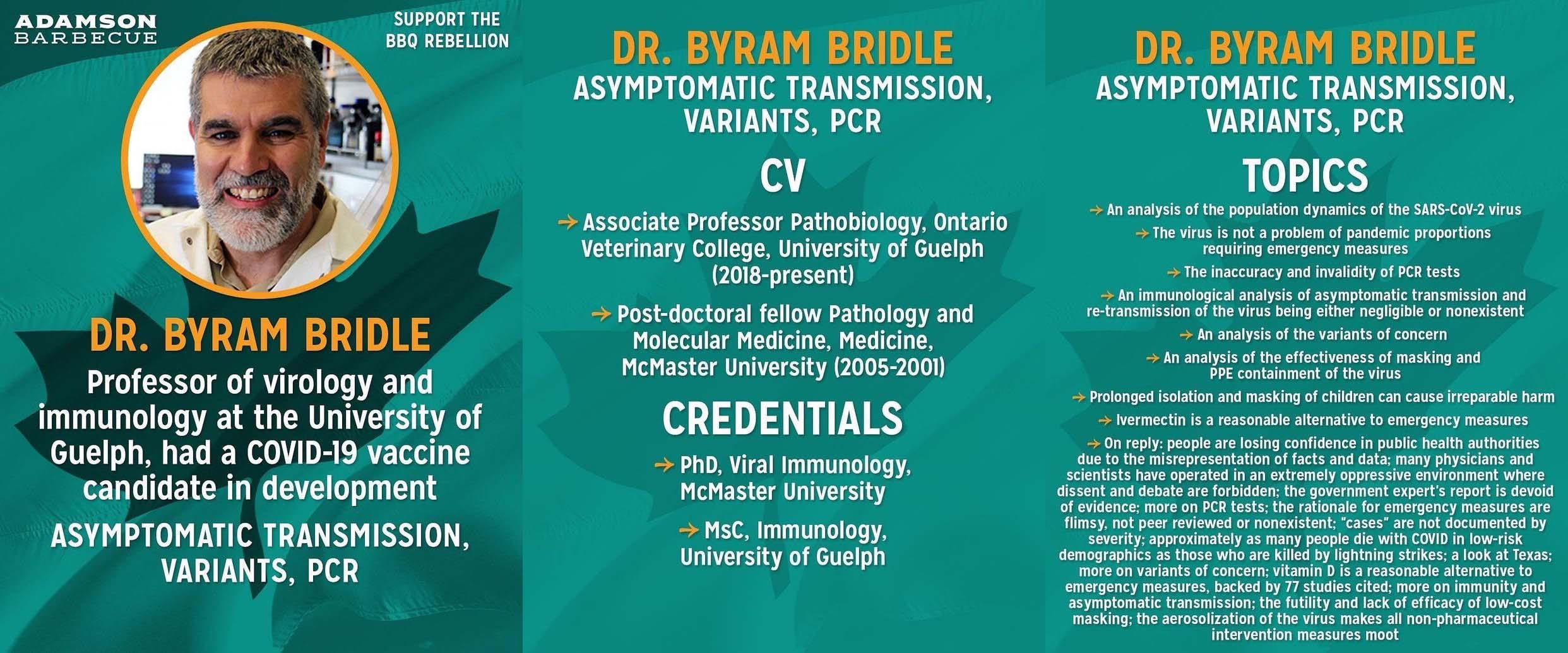
According to witness Dr. Byram Bridle, professor of virology and immunology at the University of Guelph, who reviewed the available literature on IVM in his April 2021 affidavit, “Canada should include ivermectin for early out-patient treatment for COVID-19,” because there are “multiple clinical trials from different countries saying the same thing, that the treatment works, both in the early and late stages of the disease.” Since then, there have been two meta-analyses published in the American Journal of Therapeutics supporting its efficacy against covid – one in June 2021 and one in August 2021 – and IVM is endorsed by Dr. Paul Marik, the most published practicing intensivist in the world. A real-time tracker of ivermectin results, which includes 95 studies as of February 2023, indicates that “statistically significant improvements are seen for mortality, ventilation, ICU admission, hospitalization, recovery, cases, and viral clearance.”
To be clear, neither HCQ nor IVM are panaceas that could magically eradicate all traces of covid from the earth. They are simply low-risk medications that are essential to global health, inexpensive to produce, and which if used correctly, potentially could have prevented much suffering, hospitalization, and death. But for reasons that defy logic, both the FDA and the WHO actively discouraged their use, and the media shamelessly smeared their stellar reputations.
Meanwhile, the track record of the FDA in recent years has failed to inspire confidence in their oversight capabilities. They failed to stop the opioid epidemic. They needlessly delayed and were careless in their response to baby formula issues. And appallingly, they approved a drug for Alzheimer’s disease even though it was shrouded with controversy, in addition to major revelations mere months earlier suggesting that the drug’s mechanism of action was based on fabricated research. In light of the many avoidable omissions and misleading conclusions peddled by both the media and regulators throughout covid, it behoves those formerly trustworthy institutions to stop horsing around and start acting like impartial investigators once again, presenting balanced perspectives to the public and empowering them to make informed decisions.
“As experience accrued in treating COVID-19 infections, physicians worldwide discovered that high-risk patients can be treated successfully as an outpatient… with a “cocktail” consisting of hydroxychloroquine, zinc, and azithromycin (or doxycycline)… based on the pharmacology of the hydroxychloroquine ionophore acting as the “gun” and zinc as the “bullet,” while azithromycin potentiates the anti-viral effect. Undeniably, the hydroxychloroquine combination treatment is supported by science.”
It has long been known that physical activity lowers the risk of severe outcomes from covid. However, most people rely on team sports and communal facilities for regular exercise, and those were all closed during lockdowns. This is just one more example of how so-called health policies were in direct conflict with desirable health outcomes, and it is likely why authorities were remiss to mention it while restrictions were in place. However, one thing authorities easily could have commented on was the role of vitamin D for immune support. Vitamin D is critical to overall health, especially for Canadians who are chronically vitamin D deficient. It is a ubiquitous vitamin that is widely available as a supplement, can be gained via sun exposure, and is bioavailable in many common foods. And yet, not only did they fail to mention it, but in April 2021 federal health minister Patty Hajdu childishly referred to vitamin D as “fake news.” To date, there have been hundreds of studies showing that vitamin D works to improve outcomes, and as of February 2023, a large study in Nature and a definitive meta-analysis seem to have ended any lingering doubt about it.
Looking at the big picture for treatments, what HCQ, IVM, and vitamin D have in common is that they are generic drugs, which are inexpensive and barely profitable for pharmaceutical companies. With no patent-protection, there is no corporate interest in them, and no influential lobby to advocate for trials and approvals. The opposite is true for costly drugs like remdesivir, made by Gilead Sciences.
Despite remdesivir’s lofty price tag of $3,100 per treatment course; despite an initial study into its use against covid in April 2020 resulting in 31% of participants suffering serious adverse events, including septic shock and multiple organ failure; despite the primary benefit of a subsequent larger study being relatively marginal, alleging only to improve time to recovery; despite that large study being untrustworthy because the endpoint was changed midway throughfrom improvement in mortality to time to recovery; despite a massive study from October 2020 that caused the WHO to conclude it had “no meaningful effect on mortality or other important outcomes”; despite a disproportionately high volume of reports indicating acute injuries to the liver and kidney; despite no indications that it reduced viral load; and despite failing to consult with the Antimicrobial Drug Advisory Committee (ADAC), which is a group of independent experts who normally review data with the FDA – in short, despite remdesivir’s hefty cost and insufficient evidence to suggest it was either safe or effective against covid, Dr. Fauci claimed it could set “a new standard of care” for covid treatment, and the FDA inexplicably maintained its EUA until April 25, 2022.
"Gilead and the FDA have sort of maneuvered us into a position where we're being asked to try and prove remdesivir does nothing rather than asking the usual way round, which is, ‘can the manufacturers prove it does something?'"
Out of all the missteps throughout covid, the most indefensible was the omission of natural immunity. The human immune system is a miracle. Its adaptability, endurance, and resilience have historically allowed humans to co-evolve with viruses, but its integrity must remain intact for humanity to flourish. Lest it grow weak and weary, frequent exposure to the natural microbial world is necessary, as is an acceptance that not all sickness can be avoided. Like fitness training for the immune system, the body needs practice clearing pathogens to build cellular level memories that can be used to defend against other viruses in the future. For example, in January 2022, a widely shared studyacknowledged what one defamed Canadian doctor had been touting since August 2020, that T-cells generated from exposure to the common cold play a vital role in protecting against covid.
Any doctor worth their salt recognizes the marvel of the immune system. It has been known since the Athenian plague of 430 BC that those who recover after infection gain long-lasting protection. Even Dr. Fauci knew this. On March 26, 2020, Fauci was interviewed by Trevor Noah for The Daily Show, where he said, “once you get infected, get better, clear the virus, then you’ll have immunity that will protect you against reinfection. It’s never 100%, but I’d be willing to bet anything that people who recover are really protected against reinfection.”
Untrue to his word though, Fauci went on to bet against natural immunity. In October 2021, a meeting was held between the highest-ranking US health officials, including Fauci, Centre for Disease Control (CDC) director Rochelle Walensky, and US surgeon general Vivek Murthy, where they decreed that post-infection immunity would not count as the equivalent of two vaccine doses for the sake of national health policy. Notwithstanding the sinister concept of relying on an imperfect pharmaceutical product as the decisive yardstick for health and public participation, their decision dismissed the timeless immunological principle of post-infection protection, and wrongfully presumed that the “science was settled.” By depicting the immune system as inadequate, its tremendous value was trivialized, especially for those in good health and at minimal risk. It also implied an inferiority to synthetic interventions, and by extension, a dependency on them for survival.
When that meeting took place in October 2021, there were already over 160 studies affirming the benefits of naturally acquired immunity, and many millions of people around the world had recovered from covid without any therapeutics. How else could they have recovered if not for their immune systems? And why did so many health professionals seemingly have minimal faith in immune systems? By excluding natural immunity from health policy, authorities around the world put all their eggs in one basket, gambling decades of accumulated good will and credibility on new, unconventional vaccines. Predictably, their poor risk management did not pay off. In February 2023, a milestone meta-analysis in The Lancet confirmed what should have been the default position all along – that natural immunity is robust and enduring, providing broad protection against all variants, and moreover, that it provides greater protection than vaccines. All told, the dubious approach to treating covid has exposed some crucial weaknesses of the modern healthcare industry and culture. It has grown preoccupied with expensive and underwhelming pharmaceuticals; uncritical of demonstrable regulatory bias and incompetence; underappreciative of abundant, natural, and time-tested remedies; and uninterested in the innate healing power of a well-maintained mind, body, and spirit.
“We should embrace the benefits of the development of immunity in a growing segment of the population. Right now, the only means of achieving this is by natural infection. Recent data suggests that the human body reacts no differently to this virus than to other respiratory viruses: it mounts immunity, and once achieved, the virus gets cleared and there is protection from future infection.”
– Doctors Neil Rau, Susan Richardson, Martha Fulford and Dominik Mertz. May 21, 2020.

Vaccines
There are those who believed that public health followed evidence-based science, that there were no alternatives to lockdowns, that covid was exceedingly deadly, that masks were helpful and harmless, that the benefits of preserving the healthcare system outweighed the costs to all social and economic activity, that there were no effective treatments, that natural immunity was not attainable or desirable, and that dissidents were in denial. To those who believed these to be true, it’s understandable how a vaccine could have been seen as an absolute necessity. However, had they approached this topic with some healthy skepticism, they might not have been so eager to “just get vaccinated.”
Calls for a vaccine arose mere days into the initial lockdowns, even before much was known about the true nature of covid. Tempering expectations, on March 31, 2020, the American Association of Medical Colleges (AAMC) published a reminder about past issues with rushed vaccines, urging both patience and caution with covid vaccine development. Similarly, in July 2020, then-CEO of Merck, Ken Frazier, whose company has brought more new vaccines to market in the last quarter century than all other pharmaceutical companies combined, told Harvard Business School, “I think at the end of the day, we don't want to rush the vaccine before we've done rigorous science… We don't have a great history of introducing vaccines quickly in the middle of a pandemic. We want to keep that in mind.”
Commenting on the development timeline, Dr. Gregory A. Poland, director of the Mayo Vaccine Research Group, said “from the creation of the idea to having a marketable vaccine is usually seven to 10 years or more.” This timeline was echoed in testimony to US Congress in May 2020 by Dr. Rick Bright, who later became a member of President Biden’s coronavirus advisory board, when he said “normally, it takes up to 10 years to make a vaccine.” In April 2020, Dr. Emily Erbelding, an infectious disease expert at Dr. Fauci’s NIAID, not only reiterated that the typical vaccine development timeline is eight to 10 years, but worryingly, she added that an accelerated process would involve “not looking at all the data.” A lengthy diligence process is important to minimize harms, ensure long-lasting benefits, and assess risks, some of which can take years to emerge and be understood. Prudently, Dr. Poland added, “if we aren’t deliberate and careful, we could harm people. We have to remember that.”
“If you take [a vaccine], and then a year goes by and everybody's fine, you say, OK, that's good, now let's give it to 500 people. And then a year goes by and everything's fine. You say, well then, now let's give it to thousands of people. And then you find out that it takes twelve years for all hell to break loose – then what have you done?”
For context, the AAMC explained how the initial measles vaccine in the early 1960’s didn’t protect children from measles, but made symptoms worse when they were infected, often resulting in hospitalization. Similarly, children vaccinated for respiratory syncytial virus (RSV) in the 1960’s developed an enhanced form of the disease. Sharing the same sentiment as the AAMC, CNN cautioned their readers in September 2020 that “when the vaccine making process has been rushed, there have been bad outcomes.” Among their chosen examples, they cited the initial polio vaccine from 1955, where 20% of the 200,000 injected children became infected because the vaccine contained a live virus, which killed ten and left hundreds with paralysis. They also described how in 1976, President Gerald Ford was convinced by ‘experts’ that there was a swine flu pandemic – a pandemic that never materialized – prompting him to mandate a hastily assembled vaccine. The vaccine, which did not prompt any immune response, was given to 40 million people, causing some to develop Guillain-Barre syndrome. Alas, these problems are not relegated only to the distant past.
In November 2019, the Associated Press reported that more new cases of polio in four African countries were caused by vaccines than by the wild virus. And then in March 2023, the Associated Press reported that Burundi declared a polio outbreak due to a new strain of the virus which, once again, originated from a vaccine. Even though these used an oral live virus vaccine, as opposed to the non-live vaccines offered in most developed nations, it’s frightening how 70 years since the initial polio vaccine debacle, the exact same mistake continues to occur again and again.
Looking at the impact of vaccines over extended timelines, in 2018, Danish researchers published the results of a study analyzing 30 years’ worth of records from Africa related to the inactivated Diphtheria–Tetanus–Pertussis (DTP) vaccine. What they discovered was shocking. Although the vaccine proved effective versus DTP, vaccinated children were ten times more likely to die from other health issues compared to unvaccinated children. They concluded that this DTP vaccine was associated with higher mortality, constituting a clear danger signal. What this revelation makes clear is, in the same way covid restrictions missed the forest for the trees by attempting to stop a single virus at the expense of all other determinants of health, vaccines must also be assessed in greater context. To minimize unintended consequences and ensure that the targeted benefits of vaccines markedly outweigh their broad potential costs, it is imperative that their long-term impacts are studied and compared to a control group; to the unvaccinated. With other similar danger signals emerging and confidence in vaccines declining globally, health authorities would be well-advised to thoroughly investigate this topic, lest their inaction be interpreted as a form of wilful ignorance.
As this relates to the covid vaccines, if there are many instances of vaccines initially believed to be safe and effective, which subsequently had issues after their rollouts, then why give a brand new covid vaccine the benefit of the doubt? Why rush to give it to anyone besides the vulnerable when harmful effects may be imperceptible in the short-term, taking years to materialize, and studies examining long-term risks are not available? Furthermore, why disparage and alienate anyone volunteering to remain unvaccinated, since they are the unintentional yet vital control group that will ultimately illuminate the covid vaccine’s true safety and efficacy? While it is a noble endeavour to develop products that protect against harmful viruses, there is no such thing as risk-free reward. As a category of product deemed “unavoidably unsafe” by both the US Congress and the US Supreme Court, there are undeniable costs to vaccines, and they warrant as much scrutiny as their potential benefits.
“Many people are asking, ‘Well why do we have to test the vaccines? Why don’t we just make the vaccines and give them to people?’ Well the world has learned many lessons in the mass use of vaccines and there’s only one thing more dangerous than a bad virus, and that’s a bad vaccine. We have to be very, very, very careful in developing any product that we’re going to inject into potentially most of the world population.”
– Dr. Mike Ryan, execute director of WHO Health Emergencies Programme. April 1, 2020.
In response to the early demands for a covid vaccine, on April 29, 2020, President Donald Trump offered up ‘Operation Warp Speed’ to expedite the “speed of science.” Despite the rushed timetable, many health practitioners and public officials maintained that the trials lived up to expected standards. To their discredit, in February 2023, Liberal Minister of Parliament (MP) Anthony Housefather explained why this could not possibly be the case. When opposition MPs asked to view the contracts signed by the government with vaccine manufacturers, he said “these documents were signed at the beginning of the pandemic when everybody was desperate for vaccines, when companies were being told to rush vaccine production and do testing in an unprecedented way, in a way they normally don’t do it… They didn’t do the type of testing that normally takes these drugs years to come to market.” Predictably, this ‘move fast and break things’ approach – popularized by entrepreneurs with an appetite for risk and a willingness to exchange integrity for expediency – was not well suited to vaccine development.
The first red flags appeared during the trials. After Pfizer, Moderna, AstraZeneca (AZ), and Johnson & Johnson published their vaccine trial protocols in September 2020, former Harvard medical school professor, Dr. William A. Haseltine, explained the implications of the trial designs. He pointed out that “prevention of infection must be a critical endpoint,” but that “prevention of infection is not a criterion for success for any of these vaccines.” This was subsequently confirmed by Christina Antoniou, Pfizer’s director of corporate affairs, in October 2022 when she replied to the Toronto Sun, saying “trials were not designed to evaluate the vaccine’s effectiveness against transmission of SARS-CoV-2.” Even if it was hoped that they would prevent transmission, it should have been obvious to all that they didn’t with the epidemic of so-called “breakthrough” cases shortly after the vaccines were rolled out to the public. For example, eight players on the ‘fully’ vaccinated New York Yankees caught covid in May 2021. If only one or two players caught covid, perhaps a “breakthrough” case could have been considered rare, but with over 30% of the team catching it at once, it should have been readily apparent that these vaccines were utterly incapable of stopping spread.
On the topic of reducing severe disease, Dr. Haseltine wrote, “we all expect an effective vaccine to prevent serious illness if infected. Three of the vaccine protocols – Moderna, Pfizer, and AZ – do not require that their vaccine prevent serious disease, only that they prevent moderate symptoms which may be as mild as cough, or headache.” Crucially, he also noted that “none list mortality as a critical endpoint.” Peter Doshi, associate editor of the BMJ, also observed this, writing in October 2020 that “none of the vaccine trials are designed to detect a significant reduction in hospital admissions, admission to intensive care, or death.” In other words, the vaccines did not test for the reduction of severe symptoms, hospitalization, and death. If the trials did not test for them, then on what basis did public health officials and medical practitioners claim that vaccines stopped spread, reduced symptoms, or reduced deaths? Why were they so confident promoting this product when the evidence supporting its alleged efficacy was non-existent?
Upon completion of the Phase 3 trials in late 2020, the manufacturers claimed that the vaccines were 95% effective. You may recall how that figure was parroted by every major news outlet and celebrated by the healthcare community. What wasn’t widely shared, however, was that it referred to the vaccine’s relative risk reduction (RRR). Leaving aside the technical explanation of the term, the FDA guidebook, Communicating Risks & Benefits: An Evidence-Based User’s Guide, explains how “patients are unduly influenced when risk information is presented using a relative risk approach; this can result in suboptimal decisions. Thus, an absolute risk format should be used.” In other words, according to the FDA, it is misleading to present the RRR to the public for the purpose of decision-making. And yet, that’s exactly what was done. Even worse, the recommended format for quantifying efficacy, absolute risk reduction (ARR), was a measly 0.84%. Why didn’t regulators or doctors catch this sleight of hand, which substituted RRR for ARR, and alert the public to ensure they made an informed decision about the vaccine? How many people would have taken the vaccine if they understood that it offered less than a 1% benefit?
“These studies seem designed to answer the easiest question in the least amount of time, not the most clinically relevant questions.”
– Peter Doshi, associate editor of British Medical Journal. October 21, 2020.
Shortly after the launch of Operation Warp Speed, on May 12, one official for the project spoke with the journal Science on the condition of anonymity, expressing concern that it was “heavily weighted” towards two candidates, including one made with messenger RNA (mRNA) encoding the coronavirus surface spike protein. The official acknowledged that mRNA technology had never led to an approved vaccine for any other disease. This was also noted by BioNTech, which partnered with Pfizer to create one of the mRNA vaccines for covid, in their December 2021 annual report filed with the Securities and Exchange Commission. In it, they cautioned that “mRNA drug development has substantial clinical development and regulatory risks due to limited regulatory experience with mRNA immunotherapies,” and that “mRNA product candidates represent an entirely new therapeutic modality.” That being the case, why was this technology favoured? Why was it believed to be well suited to combat covid? What mechanism of action made it compelling?
The active components of traditional vaccines are typically dead or weakened virus particles. Upon injection, they are meant to mimic a natural infection and prompt the body to mount a natural immune response. In effect, this method is predicated on the known benefits of natural immunity. The same is not true of mRNA technology. As explained on the CDC website, “mRNA vaccines use mRNA created in a laboratory to teach our cells how to make a protein – or even just a piece of a protein – that triggers an immune response.” For covid, the mRNA protein in question are spike proteins, which are a piece of the virus that facilitate the entry of viruses into our cells. In effect, the mRNA vaccines instruct our bodies to create lab-engineered virus particles, meaning the body’s response to the vaccine is manufactured, not natural. Could any unintended side effects result from such a novel process?
The rationale for this approach was outlined in an August 2020 study in Nature. It explained that vaccine induced spike proteins are designed to provoke an enhanced immune response compared to the wild virus spike proteins. Although the scientific community was understandably excited at this prospect, they may have gotten ahead of themselves because there was no mention of the spike protein’s potential downsides of this novel approach. And it wasn’t until late 2020, around the time that the vaccines began rolling out to the public, that evidence of harms from spike proteins emerged. For instance, in April 2021, one of America’s most prestigious independent research institutes, the Salk Institute, explained how the spike protein damages cells and plays a key role in illness. While their report made a point of differentiating between the wild covid spike protein from the vaccine induced spike protein, the safety of the latter appears to have been taken for granted, likely because research into it tends to focus on the benefits of vaccine induced spike proteins, not its potential drawbacks. Additionally, the safety of the lipid nanoparticles (LNP), which facilitates delivery of the mRNA into our cells, is also unsettled. There is reason to believe they may be highly inflammatory. When it comes to the safety of mRNA vaccines, authorities are not talking about the elephants in the room.
“It was counterintuitive because Pfizer was mastering, or let’s say we had very good experience, with multiple technologies that could give a vaccine… mRNA was a technology that had never delivered a single product until that day. Not a vaccine, not any other medicine, so it was very counterintuitive, and I was surprised when they suggested to me that this was the way to go.”
On October 22, 2020, Dr. Steve Anderson, director of the FDA’s office of biostatistics and pharmacovigilance, presented the FDA’s plan for monitoring covid vaccine safety. The presentation reviewed several safety surveillance strategies, including their intent to monitor the Vaccine Adverse Event Reporting System (VAERS), which is co-managed by the CDC and FDA. It also featured a working list of 22 adverse outcomes that they planned to monitor for, including:
Guillain-Barré syndrome
Acute disseminated encephalomyelitis (ADEM)
Convulsions/seizures
Stroke
Acute myocardial infarction
Myocarditis/pericarditis
Autoimmune disease
Pregnancy and birth outcomes
Disseminated intravascular coagulation (DIC)
Venous thromboembolism (VTE)
Multisystem Inflammatory Syndrome in Children (MIS-C)
Vaccine enhanced disease
Deaths
Many of these effects were mocked as conspiratorial or unrelated to the vaccine by media and health officials, but based on this presentation, the FDA had reason to suspect they could be linked from the start. Furthermore, their partner in monitoring for adverse events, the CDC, seemingly expected a high volume of reports. In August 2020, the CDC contracted General Dynamics, an aerospace and defence company, to handle the VAERS reports for covid vaccines. The contract anticipated upwards of 1,000 reports per day, with 40% being serious in nature. By March 2021, they were so backlogged that the contract was expanded to increase capacity to over 3,500 per day. This was not disclosed to the public during the vaccine rollout, and was only revealed in December 2022 after Josh Guetzkow, law professor at the Hebrew University of Jerusalem, published the relevant documents obtained through a Freedom of Information Act (FOIA) request. If the vaccines were as safe as advertised, then why did the CDC expect an influx of adverse events reports? Why were those specific adverse events being monitored for by the FDA? Did VAERS or other safety monitoring systems detect rises in those specific adverse events after the vaccination campaign began?
“Remember: You’re giving this vaccine, likely, to healthy people – who are not the people typically who are dying from this infection, so you better make sure that you are holding it to a high standard of safety.”
VAERS is by no means a perfect tool; it is merely intended to be an early warning system. To that end, it is difficult to dispute that the publicly available data contained red flags. For instance, during the five years preceding the covid vaccines, VAERS recorded an average of 492 deaths from vaccines per year. In 2021, that number increased by a factor of 45, to 22,386, with another 12,482 in 2022. There were also pronounced increases in reports of vaccine-induced myocarditis, pericarditis, stillbirths, miscarriages, and more. What is most telling about the data was that these figures increased and receded in unison with the number of doses administered, suggesting a correlation.
VAERS critics often downplay this data on the basis that submissions can be made by the public, who may produce false or misleading reports. While there have been rare instances of this, it is punishable by law to submit false claims, so there is a disincentive to do so. Additionally, false claims do not negate all the honest reports by health care providers, who are required by law to submit adverse event reports to VAERS. Unless critics are suggesting that most reports submitted by health care providers are false, the VAERS data is at worst a noisy signal warranting further investigation, such as an analysis from January 2023 by Professor Guetzkow.
If “ongoing reports of serious cardiac adverse events” was enough to revoke the EUA for a time-tested drug like HCQ, shouldn’t more than 22,000 reports of death – even if some are misattributed – be enough to at least pause vaccines with novel mechanisms of delivery and action, especially given the well-documented history of rushed vaccines? If an automobile airbag defect resulting in three deaths is enough to warrant an urgent warning to car drivers, and if chocolate can get recalled due solely to the possibility of salmonella contamination, and if cheese can get recalled due to possible listeria contamination resulting in zero confirmed illnesses, then why not vaccines? The answer: liability.
Unlike producers and service providers in every other industry – including prescription drugs – who are required by law to compensate consumers for harms caused by their products, only vaccine manufacturers get a free pass on liability. This is true of both covid vaccines and all routine vaccines. Apparently, vaccine manufacturing is the one and only exception to the rule that there’s no such thing as risk-free reward. Except, that’s not entirely true. The risks still exist, but they’re not borne by the vaccine manufacturers, nor by the governments who purchase them, nor by politicians who mandate them, nor by the public health officials who market them, nor by the regulators who approve them, nor by the doctors who administer them. Instead, the risks are transferred onto members of the public every time they roll up their sleeves.
“There are a lot of examples of vaccines in the past that have stimulated the immune system, but ultimately didn't confer protection. And unfortunately, there are some cases where it stimulated the immune system and not only it didn't confer protection, but actually helped the virus invade the cell because it was incomplete in terms of its immunogenic properties. We have to be very careful.”
– Ken Frazier, then-Chief Executive Officer of Merck. July 13, 2020.
On April 8, 2021, Dr. Seema Marwaha, a Toronto-based internal medicine specialist and editor-in-chief of Healthy Debate, told the Globe & Mail, “this is the first time I’ve been really scared during the pandemic. What I’m seeing... is younger people getting sicker in a more unpredictable way, in a way that’s more difficult to trace in much higher numbers.” Although it was not her intent, her statement implied certain inconsistencies in the predominant covid and vaccine narratives. In revealing that she was not “really scared” prior to that point, it could reasonably be inferred that there was less to fear from covid than had been advertised by health authorities. By describing how “younger people are getting sicker,” it could reasonably be inferred that the vaccine rollout, which was expected to be a boon to health, curiously coincided with a rise of sudden and unexpected illness among those who were least vulnerable. Lastly, in saying that sickness began occurring “in a more unpredictable way, in a way that’s more difficult to trace,” it could reasonably be inferred that with covid there was an established order to symptomatic covid illness, but that the effects from this outburst were more indiscriminate. So, are the covid vaccines responsible for this surge of unpredictable illness? Between the checkered history of vaccine rollouts, the rushed trials, the novel mechanisms of action and delivery, the known possibility of adverse effects, and in lieu of any other suspected causes, it would be irresponsible to rule this out.
Consider the Pfizer trial for those aged 12-15. The trial only had 2,260 participants. Half were vaccinated (the treatment group) and half received a saline injection placebo (the control group), meaning the trial was not designed to discover the risks of serious adverse events if they occurred at a frequency greater than one in 1,200, because less than 1,200 trial participants were given the vaccine. Yet sadly, the trial did find a serious adverse event, which struck a girl named Maddie De Garay. According to her mother, within hours of her second dose Maddie developed major health issues, including severe abdominal pain, swollen extremities, chest pain, tachycardia, mysterious rashes, reflux, gastroparesis, vomiting, dizziness, convulsions, menstrual changes, decreased vision, tinnitus, memory loss, extreme fatigue, and more. Are any of these the “unpredictable ways” adolescents were getting sick in early 2021?
Per the trial, Pfizer diagnosed Maddie as having experienced “functional abdominal pain,” and the investigator hired by Pfizer said he didn’t “feel” like the vaccine caused Maddie’s injury, even though she was in good health immediately prior to her second shot. Despite Maddie having to spend the rest of her life in a wheelchair, fed through a feeding tube, the FDA took Pfizer at their word, blindly accepting the investigator’s conclusion without doing any of their own due diligence. If Pfizer was willing to downplay the severity of Maddie’s reaction and the FDA was unwilling to investigate it, then what else might have they omitted or misled the public about?
Regarding the adult trials, Pfizer released its six-month report on vaccine safety and efficacy in September 2021. Leaving aside their questionable decision to unblind the study and vaccinate 19,525 of the 21,728 members (89.9%) of the control group before the planned completion of the trial in 2023, the company proudly touted a 91% reduction of positive cases. While that sounds helpful, cases are not indicative of actual symptomatic illness. More importantly though, the study revealed that vaccine recipients had a 300% increase in adverse events and 75% increase in severe adverse events compared to the control group. Moreover, there were more deaths in the vaccinated group (15) than in the control group (14), and that’s before the trial was unblinded. Another five died in the vaccinated group after unblinding. In other words, the treatment group had more illness and death than the control group. It seems reasonable that regulators would have known about this information, which Pfizer buried in the trial’s supplementary index, and subsequently alerted the public, but they either missed it, proving their incompetence, or kept silent, proving their complicity.
Adding more credence to the notion that covid vaccines might not be safe, in August 2022, an independent study published in Vaccine, a prominent medical journal for vaccines, re-analyzed both the Pfizer and Moderna trial data. The study received no funding and was authored by several noteworthy scientists, including the BMJ’s Dr. Peter Doshi. It discovered that the actual frequency of serious adverse events was one in 800, which is very high. Putting the puzzle pieces together, if there is reason to suspect that vaccines cause severe adverse events in at least one out of every 1,200 children and one out of every 800 adults, and that the vaccines can cause unexplained and unpredictable illnesses, then why aren’t more healthcare professionals expressing doubts about the vaccine? Why is it inconceivable to many that the vaccines could be causing harm?
Sadly, many doctors and healthcare professionals, as well as policymakers and politicians, prematurely jumped to the conclusion that a return to “normality” would be dependent on vaccines as early as April 2020. In effect, they bet their reputations on vaccines as the solution prior to having a sound understanding about either the virus or the vaccines. By blindly staking their credibility on a vaccine prior to completing the work required to prove its suitability, cognitive dissonance impairs them from criticizing and re-evaluating the vaccines’ presumed safety and efficacy. This cavalier ‘shoot first and don’t ask questions later’ mentality seems even more dubious since it’s been discovered that vaccine manufacturers, abetted by sluggish regulators, withheld consequential trial data. A FOIA request seeking the public disclosure of all 451,000 pages of trial data related to the Pfizer vaccine was made in August 2020, but the data was not released until January 2022, when many were already taking their third doses. With so much material data wilfully withheld from the public, how could any vaccine recipient possibly have given informed consent? Tragically, they couldn’t have.
“We’ve never had such an important clinical trial — or series of clinical trials — in recent history. Everything should be transparent.”
– Dr. Eric Topol, professor of molecular medicine at Scripps Research. September 13, 2020.
In the months and years following the mass vaccination campaign, sentiment towards vaccines has waned as experts and laymen alike have come to better understand its risks. With the benefit of hindsight, some influential voices who previously advocated for covid mRNA vaccines have completely changed their tune. To name just a few examples:
Dr. John Campbell, an independent health researcher and educator who has a YouTube channel with over 2.7 million subscribers, called to “pause the current covid-19 mass vaccine rollout program due to the risks associated with the vaccines.” He also apologized for misleading his viewers on vaccines, and admitted to being too trusting of scientific authorities and publications.
Dr. Drew, an American internist and media personality with more than 2.6 million Twitter followers, said about his vaccine advocacy, “I want to, as effusively as I can, fall on my sword… I was dismissive… I was as wrong as I can be.”
Dr. Retsef Levi, an MIT professor, former Israeli intelligence officer, and expert in risk management and health systems, said, “all covid mRNA vaccination programs should stop immediately. They should stop because they completely failed to fulfill any of their advertised promises regarding efficacy, and more importantly, they should stop because of the mounting and indisputable evidence that they cause unprecedented levels of harm.”
Dr. Aseem Malhotra, a prominent British cardiologist who promoted the vaccine on the BBC as a medical expert during covid, said “I can’t think of any drug, anything that we have ever used in medicine that has efficacy that is this poor… In the trial, you were more likely to suffer a serious adverse event from the vaccine… than you were to be hospitalized with covid during the original Wuhan strain… This vaccine should never have been approved for a single human in the first place."
There are many more doctors, scientists, analysts, researchers, pundits, and even politicians, who have re-evaluated the data and recanted their support for the covid vaccines. Even the Mayo Clinic’s Dr. Poland, a respected vaccine expert, is calling for further investigations because he is one of over 16,000 people reportedly suffering from tinnitus – a life-altering condition – due to these vaccines. To his dismay, he found the CDC to be “unconcerned” by the tinnitus reports, prompting him to publicly ask, “why has the CDC not done all of the research that they should do on this and published it?” Dr. Poland also said he believes the spike protein from the vaccine may be a contributing factor, as it is with other adverse events, which further calls into question the wisdom of instructing our bodies to create them via mRNA technology.
It may be tempting to deride skeptics and critics of these vaccines as agents of misinformation – reverting to the type of inflammatory rhetoric typical of the intellectually insecure – but an honest intellectual ought to take a genuine interest in their concerns and question them accordingly. Why did they re-visit their assumptions about a product they previously believed to be vital? What evidence persuaded them to change their minds about its safety and efficacy? Questions could also be posed to those who remained unvaccinated. Why did they approach the covid vaccines with such caution? Why didn’t they trust the so-called “scientific consensus” or the regulators? Moreover, an honest person might look in the mirror to reflect on their own assumptions and actions. Was the gratuitous promotion of vaccines, and coercion for their uptake, truly justified? Was information about vaccine trials, safety, and efficacy, transparent and straightforward? Has any new information come to light, which may not have been available during the initial rollout, which would have changed the risk-benefit analysis? Have health outcomes and mortality rates improved since the vaccines were administered? Barring any sincere introspection and reconciliation of the truth, the hubris of vaccine proponents may deservedly prompt a wholesale re-evaluation of all vaccines, not just the covid shots, as those whose trust they lost seek truth wherever else it may be forthcoming.
“Good science requires rigor, discipline, and deliberate caution. Any medical therapy approved for public use in the absence of extensive safeguards has the potential to cause harm, not only for COVID-19 prevention efforts and vaccine recipients, but also for public trust in vaccination efforts worldwide.”
The Rude Awakening
The official covid response wrapped the iron fist of absolutism inside a velvet glove of collectivism, which it used to quash all who wouldn’t comply. Top-down measures severed the lines of communication for bottom-up feedback, dismissing the unique needs, circumstances, and discoveries, of the individuals most affected by them, resulting in an immense amount of undue harm. Had it been the case that authorities initially overreacted but changed course shortly after, perhaps their actions may have been defensible. But their inability to acknowledge limitations and admit mistakes points to a bureaucracy in contempt of the rule of law, medical ethics, and the scientific method. If their negligence is swept under the rug by a submissive public eager to put the chaos of covid behind them – and perhaps too ashamed to admit any fault of their own – then the extreme tactics from this dark episode risk being legitimized, setting a dangerous precedent for the future.
When Skelly first stood his ground against public health’s encroachments, many hoped that the issues and evidence would be judged in earnest by our courts. However, over the last decade, our Supreme Court has struck a decidedly activist tone, abandoning its impartiality. This trend has continued with covid, a topic for which courts have repeatedly deferred to the ‘expert’ proclamations of public health officials, without evidence, and despite their appalling track record.
For instance, in Saskatchewan, one judge said, “I am able to conclude without the necessity of any specific proof that the possibility of contracting the Covid-19 virus poses a serious and significant health risk to people generally, including children and adults.” How could a judge jump to such conclusion without proof, especially when that very assertion was in dispute before the court? If the opinions of public officials cannot be challenged in a court of law, why are they presumed to be above reproach? In another case in Nova Scotia, the provincial Supreme Court permitted an injunction against lockdown protests on the basis that the protests displayed “a callous and shameful disregard for the health and safety of their fellow citizens.” Did the judge not understand that lockdowns also displayed a callous and shameful disregard for health? Why was covid presumed to be the only determinant of health, as opposed to a single variable in a much larger equation? In another case, the Federal Court concluded that compulsory quarantine was consistent with the “principles of fundamental justice.” How is confining the movement of people who have not committed any crime consistent with the principles of fundamental justice?
As shameful as it’s been that courts blindly accepted public health’s radical assertions about covid as gospel, the opportunity still exists to expose the misconduct of authorities by entering compelling evidence into the public record. For example, in July 2022, civilians Shaun Rickard and Karl Harrison challenged the federal vaccine mandate for plane and train travel, successfully exposing the lack of evidence underpinning the policy. During cross-examinations, Dr. Celia Lourenco, director general of the Biologic and Radiopharmaceutical Drugs Directorate within Health Canada’s Health Products and Food Branch – who had final authority on vaccine approval in Canada – acknowledged that she did not advise anyone to implement the mandate, nor was she consulted about it. Additionally, it was discovered that Jennifer Little, the bureaucrat who wrote the travel policy, did not receive any recommendation from health officials to implement it, nor did she consider its ethical implications.
After this information came to light, and before the trial was completed, the government dropped the mandate. Whether the decision was related to the case’s revelations or changes in public opinion is unknown, but one thing is for certain – it had nothing to do with science. Shortly thereafter, the judge decided that the case was moot, which set another dangerous precedent by suggesting that it’s acceptable for government to violate rights so long as it stops before anyone can hold them to account. With nobody held responsible for a harmful policy implemented based on a provably false claim, trust in public officials and institutions has deservedly eroded, and therein lies the rub.
A society that presumes sickness is inherently ill and cannot be trusted on matters of health. A society that prohibits physical activity and social connectiveness cannot be trusted on matters of well-being. A society that treats symptoms and fails to investigate root causes cannot be trusted on matters of vitality. A society that isolates its elderly and frail cannot be trusted on matters of compassion. A society that underestimates the costs of closing businesses cannot be trusted on matters of economics. A society that vilifies differences of opinion cannot be trusted on matters of tolerance. A society that withdraws when faced with risk cannot be trusted on matters of courage. A society that embraces segregation but not loved ones cannot be trusted on matters of empathy. A society that permits politicians to sow division cannot be trusted on matters of unity. A society that allows itself to be consumed by fear cannot be trusted on matters of hope. A society that abides by illiberal mandates cannot be trusted on matters of duty. A society that compels conformity at the expense of individuality cannot be trusted on matters of liberty. And a society that appeals to authority without verification cannot be trusted on matters of truth.
Society was built on a foundation of trust, but it has been well and truly broken by the cascade of systemic failures these last three years. If we are to forge a brighter future that is healthy, thriving, and brimming with optimism, those who were lulled into complacency by the false benevolence of authority must shatter the frame of subservience in their minds. There is much to be lost by succumbing to the unjust whims of busybodies who run interference from a distance, removed from the consequences of their actions; and there is much to be gained by taking personal responsibility for yourself and those closest to you.
By opening his restaurant during lockdown, Adam Skelly rightfully defied the bureaucrats who unjustly inserted themselves between consenting adults. They obstructed mutually beneficial interactions while bearing no cost for their meddling. Meanwhile, Skelly’s stand best served those whose lives his actions most affected. He served his employees, whose livelihoods were dependent on his business continuing to operate. He served his community, by attracting consumers from other regions and generating tax revenue. He served his customers, by meeting their demand for delicious, barbequed feasts. He served his family, who count on him to provide for their well-being. And of course, he served himself, by exercising his rights to satisfy his pursuit of truth, purpose, and prosperity, without infringing on the rights of others.
Adam Skelly’s saga may yet be unfinished, but this story is not about ends, it’s about means, and the means used in the failed attempt to control covid were monumentally unjust. Politicians, health authorities, media, and even the courts, are remiss to admit it, but people everywhere are waking up to the undeniable truth – covid was not a nightmare because the virus posed an existential threat to all, but because those in power abandoned the principles and violated the rights designed to protect every one of us from their overreaches. No threat, known or unknown, excuses that. Overbearing surveillance and directives to control people’s movements, gatherings, activities, livelihoods, bodies, and beliefs, are not hallmarks of a free society, but of authoritarian regimes. With the foul stench of egregious rights violations lingering among the remnants of this once glorious nation, stirring a burning desire for accountability from millions of wronged Canadians, vindication for the Barbecue Rebellion is just what the doctor ordered.
Hi Jesse. This is a beautiful article (and series of subsequent articles). It is very important to have accurate renditions of key issues related to COVID-19 enshrined in writing. I can guarantee that the people who promoted the incredibly flawed narrative are doing everything in their power to record their 'official' version for the history books. Writings like these are the ones that we really need to get into the history sections of our school libraries.
Great writing and chronological account of the horrid and unforgivable acts that occurred during the three-year Covid era...all in the name of “science” and “health.” The perpetrators must be held accountable for their lies and the harm they caused. Bravo to Adam Skelly for his courage and conviction. Immune health will never be found in isolation, a mask or a vaccine.